Why the 503A vs. 503B Distinction Is the Only Regulatory Story That Matters Right Now
503A vs 503B compounding: What patients need to know about peptide sourcing, sterility standards, and safe access
Patients are reading the headlines and drawing the wrong conclusion.
"The FDA banned GLP-1s." Wrong. "Compounded GLP-1s are gone." Wrong. "I need to find a research chemical source." Not only wrong — this is the most dangerous response available.
The FDA did something specific: it proposed permanently removing semaglutide, tirzepatide, and liraglutide from the 503B bulk compounding list. That is a meaningful regulatory action. But it is not a ban on compounded GLP-1 access. And the difference between those two statements is the difference between a patient making an informed transition and a patient making a panicked mistake.
Understanding that difference requires understanding what 503A and 503B actually mean. Almost nobody explains this clearly for patients.
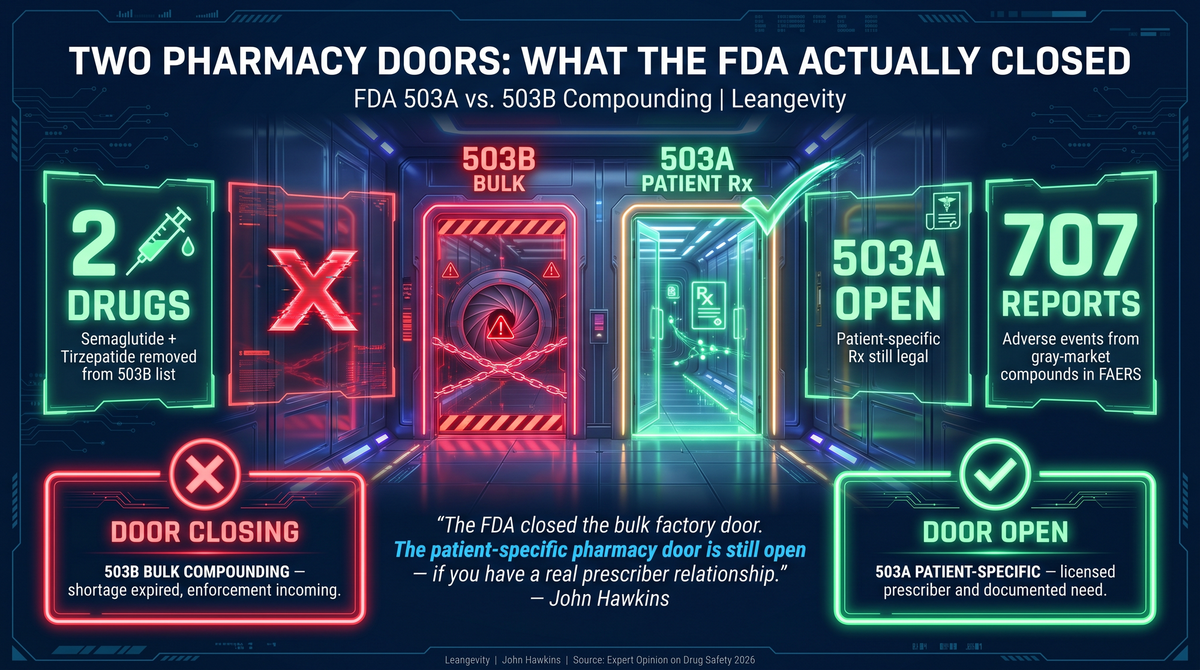
Two Doors, Not One
Pharmaceutical compounding in the United States operates through two distinct regulatory pathways. Most patients and most media coverage treat them as interchangeable. They are not.
503B is the bulk compounding pathway. These are large outsourcing facilities — think industrial-scale operations — that manufacture compounded drugs in volume, without a specific patient prescription, and ship to clinics or telehealth platforms. The FDA allows this under limited circumstances: primarily when a drug is on the shortage list and the brand-name version cannot meet patient demand.
503A is the individual prescription pathway. A patient has a unique medical need. A licensed prescriber writes a script. A local or specialty compounding pharmacy compounds that formulation specifically for that patient. This is patient-specific, not mass-manufactured. It is a different legal framework, a different scale, and a different regulatory target.
The door the FDA is closing is the 503B door.
The 503A door is still open.
What the FDA Actually Did (and Why)
On April 30, 2026, the FDA announced a proposed rule to permanently exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list. The stated rationale: no clinical need. The brand-name versions — Ozempic, Wegovy, Mounjaro, Zepbound — are no longer in shortage.
The semaglutide shortage exception expired in February 2025. The tirzepatide shortage was resolved in December 2024. Once a drug shortage ends, the legal basis for 503B compounding of that drug collapses. The FDA is enforcing that collapse.
The public comment period runs through June 29, 2026. This is not yet a final rule. But the direction is clear.
In March 2026, the FDA sent approximately 30 warning letters to telehealth companies for misleading marketing around compounded GLP-1s. Those warning letters targeted companies making claims about compounded versions that couldn't be substantiated — not patients using them through legitimate prescriber relationships.
The Safety Layer Worth Understanding
There is legitimate safety data behind the enforcement posture, but it is frequently mischaracterized.
A pharmacovigilance analysis of the FDA Adverse Event Reporting System (FAERS) covering 2018 through 2024 identified 707 adverse event reports involving compounded GLP-1 products out of 81,078 total GLP-1-related reports. The compounded product reports showed distinct patterns: higher rates of medication errors and product quality issues compared to brand-name reports. (Expert Opinion on Drug Safety, 2026.)
Additionally, researchers identified 33 unique compounded semaglutide and tirzepatide products in the FAERS dataset — products that differed in route of administration, dosing, or added ingredients. The efficacy and safety profile of many of these formulations is largely unknown because they were never tested in clinical trials.
Here is the critical nuance: none of those documented adverse events came from regulated, quality-controlled 503B outsourcing facilities operating under proper oversight. The FAERS signal reflects the broader compounded product category, including gray-market and substandard operators. This distinction matters when evaluating what the FDA crackdown is actually responding to — and it matters when evaluating where the real risk sits.
The FDA framed its action around safety and quality concerns. But the shortage has expired, the brand-name market is fully supplied, and the enforcement timeline tracks closely with patent protection interests. Both things can be true: real quality problems exist in the compounded GLP-1 market, and the timing of enforcement is convenient for Novo Nordisk and Eli Lilly.
What This Means for Patients Currently on Compounded GLP-1s
If you are currently using a compounded GLP-1 through a telehealth platform or online clinic sourcing from a 503B outsourcing facility, your supply chain is at risk. That pipeline is what the proposed rule targets.
You have options. They are not complicated, but they require a conversation with a prescriber — not a Google search and a credit card.
Option 1: Brand-name transition through a prescriber. Ozempic, Wegovy, Mounjaro, and Zepbound are all available. Insurance coverage and prior authorization processes are the obstacle for most patients. This is navigable with the right prescriber and some persistence.
Option 2: 503A pharmacy through a legitimate prescriber relationship. If you have a documented unique medical need — a specific dosing requirement, an ingredient sensitivity, or a combination formulation not available commercially — a 503A pharmacy can still compound for you with a valid prescription. This pathway remains legal. It is not being targeted. The requirement is a real prescriber relationship and a documented clinical rationale.
Option 3: Work with a clinical program already positioned for the transition. Some programs are already ahead of the rule — they have established pharmacy relationships, transition protocols, and the infrastructure to manage the shift before the final rule lands. Getting into one of those programs now is better than scrambling after the rule is finalized.
What is not an option: gray-market research chemical suppliers. The "research use only" loophole that some suppliers have used to sell peptides without clinical oversight is closing rapidly. Patients who have been sourcing compounds this way face escalating legal and health risk. This is not a path forward.
Why the Muscle Question Gets Harder During a Transition
The regulatory noise around 503B is distracting from a clinical reality that matters regardless of which door you walk through.
GLP-1 therapy causes weight loss. Up to approximately 40% of that weight loss may come from lean body mass rather than fat mass when there is no structured support program in place. That is not a feature. That is a metabolic problem — particularly for patients over 40, where lean mass preservation is directly tied to long-term metabolic rate, insulin sensitivity, and functional capacity.
A 2026 study in Cell Reports Medicine found that GLP-1-associated lean body mass reduction did not necessarily correspond to loss of skeletal muscle function — grip strength and maximal voluntary contraction remained intact in their cohort. That is a partial reassurance.
But an Omada Health study found that GLP-1 therapy combined with a structured program produced approximately three times greater muscle mass increase compared to GLP-1 therapy alone. Three times. That is not a rounding error. That is the value of the support structure.
The transition period — when patients are changing sources, adjusting doses, or switching to brand-name formulations — is exactly when metabolic oversight becomes most important. Dose adjustments affect appetite suppression. Appetite suppression affects protein intake. Protein intake determines whether you lose fat or muscle.
This is where the coaching layer becomes clinically relevant, not just convenient.
What Both Sides Get Wrong
The FDA loyalist framing says this is patient protection — the agency stepped in because compounded GLP-1s were causing harm. That framing is incomplete. The shortage that justified 503B compounding has expired. The enforcement action follows patent restoration, not a documented safety crisis from regulated outsourcing facilities.
The peptide-bro side says access is gone, the government is restricting your freedom, and you should find alternate sources. That framing is both wrong and dangerous. 503A is not gone. Individual prescription compounding is not going anywhere. The push toward gray-market sources creates the very safety problems the FDA keeps pointing to.
Patients are caught between two bad narratives and need a third one: what is actually changing, what stays the same, and what the real decision points are.
The Actual Decision Tree
Here is what matters if you are affected:
1. Are you currently on a brand-name GLP-1? Nothing changes for you. Your prescriber manages continuity as usual.
2. Are you on a compounded GLP-1 from a telehealth platform? Evaluate whether that platform is sourcing from a 503B facility. If yes, you have a transition window before the final rule. Use it to establish a real prescriber relationship.
3. Do you have a unique medical need for compounding? A specific dosing requirement, an ingredient sensitivity, or a formulation not commercially available? Talk to your prescriber about 503A pharmacy access. That pathway is intact.
4. Are you considering switching to a research chemical supplier? Do not. The legal and safety exposure is increasing, not decreasing. This is not a viable transition strategy.
5. Do you have structured metabolic support in place? If you are on GLP-1 therapy and do not have a muscle preservation and protein intake protocol, the transition period is the time to build one. The medication creates the metabolic conditions. The program determines what happens to your body composition.
The regulatory story is about access. The clinical story is about what you do with that access once you have it.
Both doors exist. One is closing. The other is open.
The patients who come through this well are the ones who understand the distinction — and who have a prescriber and a structured program before the final rule lands.
Leangevity provides coaching and education only. This content does not constitute medical advice. For clinical evaluation and prescriptions, work with a licensed physician directly. Consult your physician before changing any treatment.
Sources: FDA proposed exclusion of semaglutide, tirzepatide, and liraglutide from 503B bulks list (fda.gov, April 30, 2026, comment deadline June 29, 2026); FAERS pharmacovigilance analysis of compounded GLP-1 adverse events 2018–2024, Expert Opinion on Drug Safety 2026 (fda.gov); FDA semaglutide shortage expiration February 2025 (fda.gov); FDA tirzepatide shortage resolution December 2024 (fda.gov); FDA warning letters to telehealth companies March 2026 (fda.gov)
For more on the clinical context of GLP-1 therapy and metabolic support, read the full guide at https://blog.leangevity.fit/503a-vs-503b-compounding