They Announced 19 Peptides on Joe Rogan. Nothing's Changed.
RFK Jr. announced 19 peptides on Joe Rogan, but FDA reclassification has not happened yet. Here is the actual GLP-1 and non-GLP-1 peptide timeline.
In February, RFK Jr. sat down with Joe Rogan and announced that the FDA would be reversing restrictions on 19 peptides. The clip got shared tens of thousands of times. Peptide forums lit up. People started asking where to order.
Nothing has changed.
Not yet. And the way that sentence lands on you — whether you feel relief or frustration — tells you exactly which camp you're in. Both camps are making the same mistake.
The actual story is more specific, more useful, and almost completely missing from the coverage. There are two separate regulatory stories happening at the same time. They affect different people, through different mechanisms, on different timelines. Getting them confused is going to cost some of you.
Let's separate them.
What RFK Jr. Actually Said — And What That Means Legally
On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. appeared on Joe Rogan Experience episode 2461. He announced that the FDA planned to return approximately 14 of 19 compounds currently listed as Category 2 restricted substances back to Category 1 — which would restore the legal pathway for licensed compounding pharmacies to make them available under physician supervision.
That's a real announcement. The coverage of it was mostly accurate at the headline level.
Here's what the coverage missed: political announcements are not rules. They are regulatory direction signals.
No Federal Register notice has been published. No proposed rule exists. The formal rulemaking process — in which the FDA publishes a proposed rule, accepts public comments, reviews those comments, and publishes a final rule — has not started. Until it does, and until a final rule is published, every compound on that list remains Category 2.
If you're buying peptides right now based on the Joe Rogan announcement, you're acting on a signal, not a law. That's a meaningful difference.
The Two Stories Happening Simultaneously
The peptide regulatory landscape right now is a bifurcated story. Two things are happening. They are not connected. Most coverage treats them as one.
Story One: GLP-1 bulk compounding is being shut down.
The FDA has proposed permanently removing semaglutide, tirzepatide, and liraglutide from the 503B bulk compounding list. The public comment period closes June 29, 2026. This is GLP-1 enforcement — the most aggressive in the agency's history. The GLP-1 drug shortage that created the compounding exception is officially over. Novo Nordisk and Eli Lilly have won back market exclusivity for now.
Story Two: Non-GLP-1 peptides may be returning to legal access.
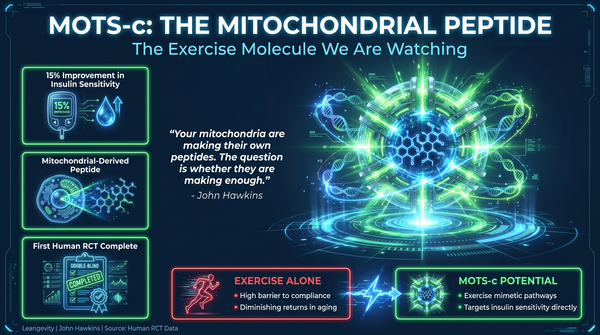
The FDA's Pharmacy Compounding Advisory Committee is scheduled to convene July 23–24, 2026. The agenda includes BPC-157, KPV, TB-500, MOTS-c, Emideltide, Semax, and Epitalon — seven compounds currently in Category 2. Around 14 of 19 Category 2 compounds are under review for potential reclassification back to Category 1. PCAC docket: FDA-2025-N-6895 (fda.gov).
These two stories share a general subject — FDA peptide regulation — but that is where the similarity ends. They are different enforcement mechanisms, different legal pathways, different affected populations, and different timelines. Conflating them is how you end up acting on the wrong information.
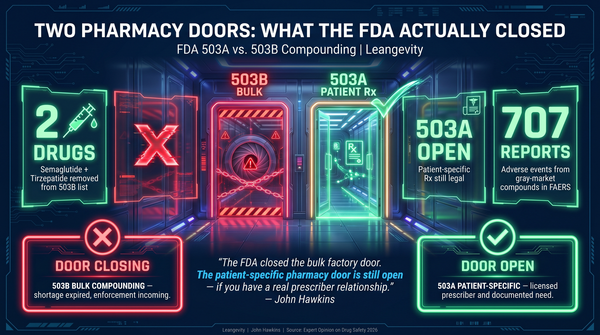
The 503A/503B Distinction That Actually Matters
This is the piece of context most people are missing, and it changes the practical meaning of both stories.
503B refers to large-scale outsourcing facilities. These compound standardized batches of medications for wholesale distribution to physicians, clinics, and hospitals. When the GLP-1 shortage was active, 503B facilities had explicit legal authority to compound. Now that the shortage is resolved, that authority is being revoked. The enforcement action is specific to 503B.
503A refers to patient-specific compounding pharmacies. These are licensed community pharmacies that prepare individualized formulations under individual prescriptions. They exist for patients who need something a commercial product can't provide — a different delivery method, an allergen-free preparation, a custom dose for a specific medical need. 503A pharmacies compound patient by patient.
The GLP-1 crackdown targets 503B. It does not eliminate 503A.
If you are a patient who genuinely cannot use a commercial GLP-1 — because the standard formulation doesn't work for your situation and a physician has documented that — a 503A pharmacy can still compound for you. That pathway has not been closed. What's closing is the shortcut: large-scale bulk compounding that was functioning as a workaround to commercial pricing.
503A is not going anywhere.
What Category 2 Actually Means — And What It Doesn't
This distinction keeps getting lost.
Category 2 is not a verdict that a substance is dangerous. It is a regulatory designation reflecting that the FDA determined there was insufficient evidence regarding safety, quality, or manufacturing standards to permit compounding. The FDA Federal Register notice from September 2023 did not cite a single documented adverse event from regulated, licensed pharmacy-compounded peptides. Zero adverse event reports from 503A or 503B facilities. The concerns were theoretical — risk profiles for immunogenicity, potential manufacturing impurities, limited human clinical data.
The 2023 ban was not based on a documented record of patient harm from regulated compounding.
Category 1 is not FDA approval. Moving a compound from Category 2 to Category 1 does not mean the FDA has reviewed it as a drug, tested it in Phase 3 trials, or approved it for a specific medical indication. It means compounding pharmacies are permitted to include it in their inventory for physician-prescribed individualized preparations. That is a narrower thing than approval. It is not a green light for mass production or direct-to-consumer sales.
BPC-157, to use a well-known example: 544 research articles published between 1993 and 2024. Preclinical toxicology data showing zero acute toxicity across multiple animal models — rats, mice, rabbits, and dogs — in a comprehensive review (Sikiric et al., Toxicology Research and Application, 2020). Phase 1/2 human trials for ulcerative colitis conducted in Croatia. No completed Phase 3 trials. No FDA approval.
Strong preclinical safety signal. Limited clinical data. If PCAC recommends reclassification and the FDA follows through, BPC-157 becomes legally available through a physician-supervised compounding pathway. It does not become an approved drug.
That's a real difference.
What the July Advisory Panel Is and Isn't
The PCAC meeting on July 23–24, 2026 is an FDA external advisory panel review. Seven peptides are on the docket.
What the panel does: it reviews evidence and makes non-binding recommendations to the FDA.
What the FDA does with those recommendations: whatever it decides. The FDA is not bound by PCAC output. It can accept recommendations, modify them, or reject them entirely. After the advisory panel concludes, the FDA must still publish a proposed rule, accept public comments, and publish a final rule before any reclassification takes legal effect.
Even if every peptide on the July docket receives a positive PCAC recommendation, legal compounding access does not resume automatically. Formal rulemaking takes time. Even fast-tracked.
A second PCAC meeting covering LL-37, GHK-Cu, Dihexa acetate, Melanotan II, and Pegylated MGF is scheduled before the end of February 2027. The 14 peptides are not all on the same timeline.
The Part Nobody Wants to Hear About the Gray Market
When Category 2 was published in September 2023, the peptides didn't disappear. The legitimate supply chain disappeared. What replaced it was a gray market: research-use-only (RUO) products from unverified overseas suppliers, sold on websites as "research chemicals," moving through Telegram groups and gym locker rooms.
The FDA has since documented the predictable results. A warning letter to USApeptide.com in February 2025 for selling semaglutide and tirzepatide as research chemicals sourced from unknown manufacturers. An FDA notification in September 2025 about Agebox iKids Growth Day Formula, in which laboratory analysis found ibutamoren — a growth hormone secretagogue — hidden in a product marketed for children.
Those are the documented cases. The undocumented cases don't get tracked because no one is monitoring unregulated supply chains.
If you are currently sourcing peptides from a research chemical website, you are operating in a loophole. The day reclassification is finalized and formally published, FDA and DEA enforcement against RUO sellers will escalate significantly. These sellers will not receive warning letters. Arrests, prosecution, and criminal liability are the realistic outcomes. The only viable path forward, when reclassification does go through, is regulated 503A pharmacy compounding under physician supervision — with sterility verification, batch testing, and a legitimate prescription.
The regulatory window is opening. It is not open yet. And when it does open, it opens through the legitimate channel.
What This Means If You're a Patient Right Now
If you're on a compounded GLP-1: Review your sourcing. If your telehealth provider is claiming a shortage exception for semaglutide, that exception expired February 2025. Ask specifically whether your pharmacy is a 503A facility with patient-specific prescriptions or a 503B outsourcer under an expired shortage designation.
If you're interested in non-GLP-1 peptides like BPC-157: The regulatory window is opening, not open. PCAC reviews begin July 2026. The formal rulemaking process takes time after that. The correct move is to work with a physician who tracks the regulatory process and can prescribe through a legitimate 503A pharmacy when access is restored.
If you're buying from research chemical websites right now: The window for legal consequence is narrowing, not widening. The announcement did not legalize research-use-only sales. It announced an intent to initiate a formal review process. Those are different things.
Both Sides of This Debate Are Wrong
This is the consistent failure in peptide coverage: people force a nuanced regulatory story into the framing they already believe.
FDA loyalists treat Category 2 as evidence that the FDA reviewed these compounds and found them dangerous. The record shows otherwise. The safety concerns were theoretical. The ban created a less-safe market than the one it replaced.
Peptide enthusiasts treat the JRE announcement as a green light — as though HHS saying they intend to reclassify is the same as having reclassified. No formal rule exists. The enforcement environment has not changed. Buying from gray-market suppliers now, on the basis of an announcement, is acting on a signal that has not become law.
The accurate read: two separate regulatory actions are underway. One is closing a GLP-1 bulk manufacturing loophole. The other is beginning a formal review process that may, over 12 to 18 months, restore legal compounding access for specific non-GLP-1 peptides through physician-supervised pharmacy channels.
Both of those things can be true at the same time without contradicting each other.
The research-use-only loophole is closing, not opening. The regulated pharmacy channel is opening, not closing.
Those are two different things for two different people. Understanding which one you are is the whole point.
Leangevity provides metabolic health coaching, not medical treatment. This is not medical advice. Consult your healthcare provider before starting, stopping, or changing any medication or supplement protocol.
Sources: FDA proposed removal of semaglutide, tirzepatide, liraglutide from 503B bulk list (fda.gov, public comment deadline June 29, 2026); PCAC Meeting Docket FDA-2025-N-6895 (fda.gov, July 23–24, 2026); RFK Jr. JRE Episode 2461, February 27, 2026; BPC-157 preclinical toxicology review — Sikiric et al., Toxicology Research and Application, 2020; NYT, March 31, 2026; WaPo, April 15, 2026.
Ready to build a metabolic foundation that makes the most of whatever tools become available? https://blog.leangevity.fit/