You're Getting Two Lies About Seed Oils. Here's the Biochemistry Both Sides Are Hiding.
The seed oil debate is stuck between institutional reassurance and biohacker panic. The biochemistry points to a more precise answer: dose, source, oxidation, and omega-6 to omega-3 ratio.
The internet has two opinions about seed oils. Either they are heart-healthy polyunsaturated fats endorsed by every major nutrition institution — or they are industrial toxins slowly destroying your mitochondria and making you fat. One camp quotes the American Heart Association. The other quotes lifespan studies in rats.
Both camps are wrong. Not partially wrong. Wrong in the specific ways that matter most for your metabolism.
Here is what the biochemistry actually shows — including the evidence each side refuses to talk about.
The Case Against Seed Oils (The Parts That Are Actually Right)
Before dismissing the anti-seed-oil crowd as internet contrarians, look at what they get right.
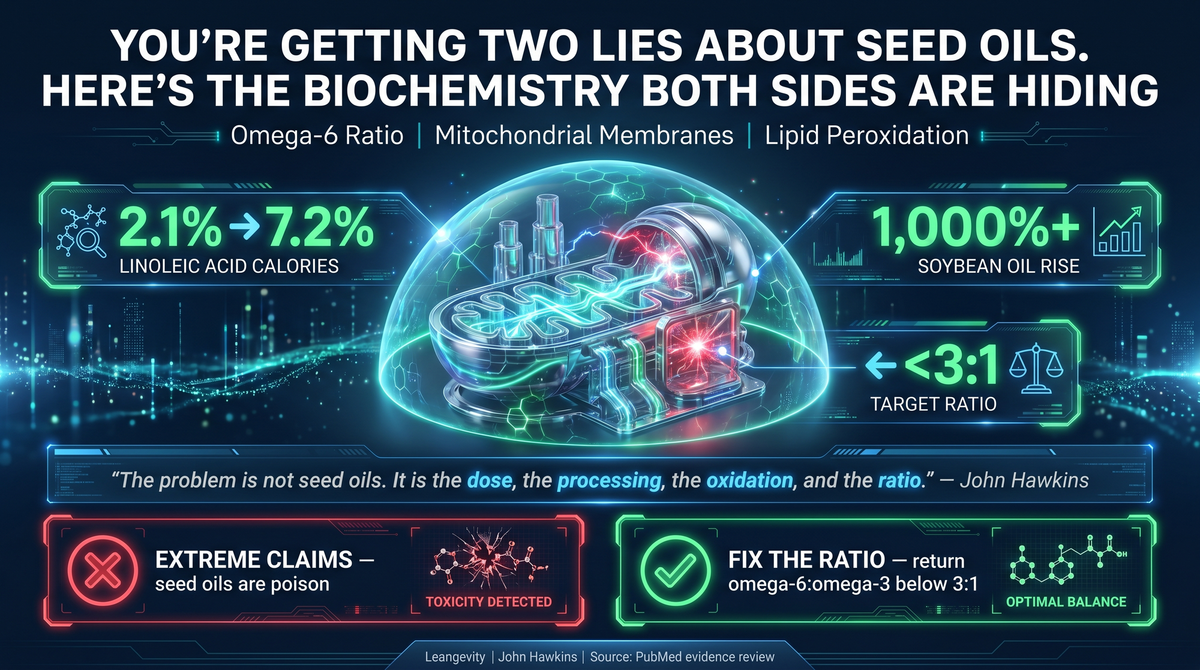
In 1909, linoleic acid — the primary omega-6 fatty acid in industrial seed oils — made up about 2.1% of American caloric intake. By 1999, it was 7.2%. Soybean oil consumption increased more than 1,000-fold during that same period. That is not a rounding error. That is a complete restructuring of what Americans eat at the cellular level. (PMID 21367944)
Your omega-6 to omega-3 ratio went from roughly 2.3:1 to 10:1. The consequences of that shift are not hypothetical — the omega-6 to omega-3 ratio determines which type of eicosanoids your cells produce. Linoleic acid converts to arachidonic acid, which converts to prostaglandins (PGE2), leukotrienes (LTB4), and thromboxanes — all potent pro-inflammatory mediators. This is not fringe biology. This is standard biochemistry, confirmed in human tissue. (PMID 29610056, PMID 24962583)
Now for the mitochondrial piece. The inner mitochondrial membrane contains a unique phospholipid called cardiolipin. It is essential for the electron transport chain to function — without properly structured cardiolipin, Complexes I through V cannot form the supercomplexes needed for efficient ATP synthesis. We know this from Barth syndrome, a genetic defect in cardiolipin remodeling that causes severe cardiomyopathy in children. That is Grade A human evidence for the cardiolipin-energy connection. (PMID 16442164)
Cardiolipin must be enriched with linoleic acid to function. That is also true. But this is where the story gets complicated.
When cytochrome c — an electron carrier inside your mitochondria — interacts with cardiolipin, it activates as a peroxidase. It selectively oxidizes polyunsaturated cardiolipin. This is the upstream event in mitochondrial permeabilization. The same molecule that makes cardiolipin functional also makes it a peroxidation target. (PMID 16408039)
When oxidized LA metabolites accumulate — specifically OXLAMs, oxidized linoleic acid metabolites — the damage becomes visible in human tissue. NASH patients (non-alcoholic steatohepatitis) show a distinct plasma lipidomic signature. Mouse models fed OXLAMs directly develop hepatic mitochondrial dysfunction, hepatocyte apoptosis, and NLRP3 inflammasome activation. (PMID 30084831, PMID 19937697)
PUFA-enriched LDL is measurably more susceptible to oxidation in human patients with type 2 diabetes. The more polyunsaturated your LDL, the faster it oxidizes when exposed to copper in vitro — which is a reasonable proxy for oxidative stress in arterial walls. (PMID 11757082)
This is the legitimate science behind the anti-seed-oil position. It is real, it is mechanistically sound, and anyone who dismisses it wholesale has not read the research.
The Case for Seed Oils (The Parts That Are Also Right)
Now for what the anti-seed-oil crowd refuses to acknowledge.
Linoleic acid is an essential fatty acid. Your body cannot synthesize it. Eliminate it entirely and you develop essential fatty acid deficiency — a clinically recognized condition with documented symptoms including dermatitis, impaired wound healing, and immune dysregulation. The question is not whether you should consume it. The question is dose, source, and oxidation state.
More importantly: the 2026 UK Biobank study (one of the largest prospective dietary datasets in existence, PMID 41617088) found that LA is associated with LOWER cardiometabolic risk. Not higher. Lower. A 500,000-person cohort giving you the opposite of what the seed-oil-is-poison crowd predicts. That is Grade A contradictory evidence, and it demands an explanation rather than dismissal.
Here is the explanation the research actually supports: native LA, at non-excessive doses, is not the same as oxidized LA metabolites. The disease data points consistently at the oxidized form — OXLAMs — as the driver of pathology, not unprocessed linoleic acid from whole food sources.
Omega-6 fatty acids also produce pro-resolving mediators. Lipoxin A4 and resolvins are derived from the same omega-6 pathway. The narrative that omega-6 equals inflammation is factually incomplete. The actual story is context-dependent, dose-dependent, and depends heavily on the competing presence of omega-3 fats. (PMID 40320870)
The two most frequently cited randomized trials against LA replacement — the Sydney Diet Heart Study and the Minnesota Coronary Experiment — are real data and deserve scrutiny. Ramsden's re-analysis of recovered unpublished data found that replacing saturated fat with safflower oil or corn oil did NOT reduce mortality. In the Sydney trial, the LA group had HIGHER all-cause mortality. In Minnesota, cholesterol dropped but mortality did not. (PMID 23386268, PMID 27071971)
That is not nothing. These are the trials that informed dietary guidelines, and the mortality data was initially unpublished. Those data deserve a public reckoning.
But here is the caveat the anti-seed-oil camp ignores: these were trials in specific clinical populations, conducted in the 1960s and 1970s, using dietary interventions that included margarine and industrial cooking oils. What they do not show is that a person eating whole-food omega-6 sources — eggs, nuts, small amounts of cold-pressed oil — is poisoning themselves. The trial data is about industrial LA replacement at clinical doses in institutionalized patients. Context matters.
What Neither Side Will Tell You About the Mechanism
The cardiolipin paradox is the most intellectually honest way to frame the seed-oil story.
Cardiolipin needs linoleic acid to function. It cannot do its job in the mitochondrial membrane without being LA-enriched. But the LA enrichment simultaneously makes it a peroxidation target. When cytochrome c activates as a cardiolipin-specific peroxidase, it degrades the very molecule the mitochondria depend on. (PMID 16408039, PMID 16442164)
Think of it as a maintenance problem at the factory level. The equipment requires a specific material to run efficiently. The supplier provides that material. But that material also degrades when exposed to the oxidative heat of normal operation. At low doses and under normal conditions, the degradation is managed and repaired. When the dose increases — when 20% of your daily calories are coming from refined industrial oils that have been heated, processed, and oxidized before they even reach you — the degradation outpaces repair.
This is not "seed oils are poison." This is dose-dependent, source-dependent, and oxidation-state-dependent risk. That is a more complicated story. It is also the honest one.
The biochemical claim that PUFA peroxidation is dangerous at body temperature (37°C) is solid. More double bonds mean exponentially more susceptibility to oxidation. DHA is roughly eight times more peroxidizable than LA. The membrane pacemaker theory — which correlates peroxidizability index with lifespan across mammals — shows that animals with more unsaturated membranes have shorter lifespans at the species level. (PMID 9788245, PMID 29610056)
What the anti-seed-oil camp extrapolates from there — that dietary PUFA suppresses thyroid function, lowers metabolic rate through proton leak, or caused the obesity epidemic through a direct causal mechanism — goes beyond what the human evidence supports. The thyroid suppression claim is animal-only. The proton leak/metabolic rate claim is preclinical. The obesity-causation claim is ecological correlation with substantial confounders.
The Claims That Do Not Hold Up
To be direct about what the evidence does not support:
PUFA does not suppress thyroid function in humans. There is no human evidence for this. The animal studies are interesting hypotheses, not clinical conclusions.
Industrial seed oils did not uniquely cause the obesity epidemic. Soybean oil consumption and obesity rates have tracked together, but so did sugar consumption, refined carbohydrate availability, sedentary lifestyle, environmental chemical exposure, and the industrialization of the entire food supply. Correlation at the population level is not causation.
The mitochondrial damage from seed oils is not "bioenergetic collapse." The Complex IV effect documented in aged rat brain mitochondria was described in the original research as "marginal." That is not a catastrophic failure — it is a quantifiable but modest impairment. Scaling from "marginal Complex IV decline in aged rat brain" to "seed oils are collapsing human cellular energy production" is not a move the data supports. (PMID 17331620)
What the Research Actually Tells You to Do
The problem isn't seed oils. It's the ratio.
For most of human history, people consumed omega-6 and omega-3 fatty acids at roughly a 2:1 or 3:1 ratio. Your body evolved around that balance. The inflammatory and anti-inflammatory pathways downstream of these fats were built for it.
The standard American diet now runs closer to 15:1 — or higher. That isn't a minor dietary tweak. That's a biochemical environment your mitochondria have never seen before, and they're not handling it quietly.
You don't have to throw out your olive oil or become a carnivore ideologue to fix this. The target is simple: get your omega-6 to omega-3 ratio back under 3:1. That means dramatically reducing industrial seed oil consumption — the soybean, corn, cottonseed, and sunflower oils baked into virtually every processed food — and cutting out anything deep-fried in those oils entirely. It means reading labels. It means going back to the fats your grandparents cooked with: butter, tallow, and animal-based saturated fats that humans have eaten for millennia without a cardiovascular epidemic to show for it. Tallow isn't going to kill you. Butter isn't going to break your heart. The seed oil-laden processed food supply might, though — not because any one ingredient is poison, but because the cumulative ratio has drifted so far from what your biology expects that inflammation has become the background noise of modern life.
This isn't about demonizing a macronutrient. It's about recognizing that dose and ratio are everything in biology. Linoleic acid isn't inherently toxic. But 10 to 15 times more of it than your cells were designed to handle? That's a different conversation entirely.
Fix the ratio. That's it. That's the intervention.
Leangevity's position on this is simple: the conversation about what you eat daily is more important than most people give it credit for. If you are eating clean, exercising consistently, and still feel exhausted, foggy, or stuck — the quality of your metabolic inputs deserves a real evaluation. That is what metabolic health coaching addresses.
If you want to understand what this looks like in practice for your specific situation, the first step is a conversation. Book a free discovery call at leangevity.fit.
Educational content only. Not medical advice. Individual results vary. Consult your physician before making any changes to your diet or treatment plan.
Sources: PMID 21367944 (Blasbalg et al., Am J Clin Nutr, 2011) | PMID 29610056 (Innes & Calder, 2018) | PMID 24962583 (Hester et al., 2014) | PMID 16442164 (Hauff & Hatch, 2006) | PMID 16408039 (Kagan et al., Nat Chem Biol, 2005) | PMID 30084831 (Schuster et al., 2018) | PMID 19937697 (Puri et al., 2009) | PMID 11757082 (Scheffer et al., 2001) | PMID 41617088 (Sala-Vila et al., 2026) | PMID 40320870 (Kaviani et al., 2025) | PMID 23386268 (Ramsden et al., BMJ, 2013) | PMID 27071971 (Ramsden et al., BMJ, 2016) | PMID 9788245 (Pamplona et al., 1998) | PMID 17331620 (Sen et al., 2007)