The FDA Is Shutting Down One Peptide Market and Opening Another
Most coverage treats peptide regulation as one story. The reality is bifurcated: GLP-1 copycat compounding is being crushed, while 14 other peptides are being reviewed for restored legal access.

Here's what's actually happening with peptide regulation right now — and why most of the coverage has it backwards.
The story isn't "peptides are banned." The story is that the FDA is executing a bifurcated policy: GLP-1 copycat compounding is being crushed with the most aggressive enforcement in the agency's history, while simultaneously the door is opening for 14 other restricted peptides — BPC-157, KLOW, TB-4 fragments, Thymosin Alpha-1 — to be restored to legal compounding status.
That's a meaningful difference. And it changes what you should do right now.
The Two Separate Cracks
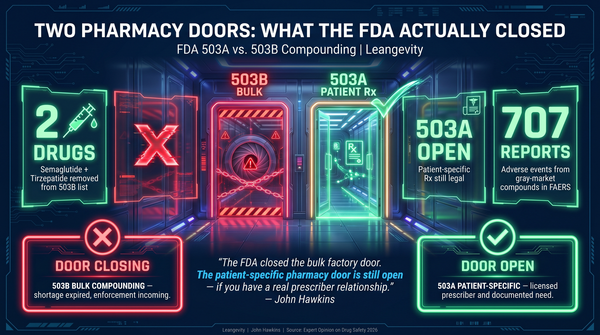
Crack #1: GLP-1 Compounding Is Being Shut Down
This is not ambiguous. The enforcement has been specific and escalating. And the clinical stakes are significant — tirzepatide, the next-generation GLP-1/GIP dual agonist, has demonstrated statistically significant benefits across 10 health domains in a meta-analysis of 17 RCTs (N=25,847): cardiovascular, heart failure, renal, MASH, OSA, blood pressure, lipids, quality of life, body composition, and inflammation — independent of weight loss (PMID 42061648, Endocrine Practice, April 2026).
That broader therapeutic profile raises the stakes for patients who may lose access to compounded GLP-1 formulations.
- March 3, 2026: FDA issued 30 warning letters to telehealth companies marketing compounded GLP-1s — the largest single enforcement action against peptide compounding in history
- April 1, 2026: FDA published formal policy clarification targeting equivalence claims and misleading sourcing from third-party pharmacies
- Salt forms of semaglutide, retatrutide, and cagrilintide explicitly prohibited from compounding
- The semaglutide shortage exception expired February 2025. The grace period is over.
The violations targeted were specific: claiming compounded GLP-1s are equivalent to FDA-approved drugs, implying telehealth companies compound in-house when they use 503A pharmacies, using the B-vitamin addition workaround to reclassify formulations as "different products." The FDA has that workaround on its radar now and is actively challenging it.
If you're on a compounded GLP-1 through a telehealth service, you should be asking hard questions about your sourcing and your compliance position. That's risk management, not alarmism.
Crack #2: 14 Peptides Are Being Reclassified From Category 2 to Category 1
This is the part mainstream coverage gets wrong by treating it as the same story.
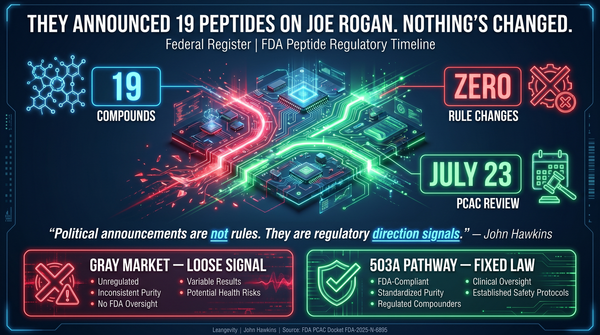
On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced on the Joe Rogan Experience (episode 2461) that the FDA would reverse the September 2023 Category 2 designation for 14 of the 19 restricted peptides. NYT confirmed the plan March 31. WaPo reported April 15 that federal officials plan to begin the review process "this summer."
Here's the nuance that matters — and that most coverage glosses over:
- No formal reclassification has occurred. No Federal Register notice exists. No PCAC review scheduled. All 14 peptides remain Category 2 today.
- PCAC reviews don't start before July 2026 at earliest. FDA is not bound by PCAC recommendations — the agency can and does diverge from advisory committee input.
- The formal rulemaking process takes 1-2+ years minimum. HHS announcements are regulatory direction signals, not current law.
The regulatory window is opening. It's not open yet. That's a meaningful distinction when your health and your legal exposure are on the line.
What the 2023 Ban Actually Did — And Didn't Do
When the FDA moved 19 peptides to Category 2 in September 2023, the stated rationale was "risk for immunogenicity, peptide-related impurities, and limited safety-related information." That's the official position from the FDA Federal Register notice.
Here's what most coverage skips: the FDA did not cite a single documented adverse event from regulated, pharmacy-compounded peptides. No contamination cases from licensed 503A or 503B facilities. No patient harm record. No emergency room data showing peptide-related injuries from pharmacy-sourced products.
The safety concerns were theoretical. Not observed in practice. From the regulated sources the ban was targeting.
Predictably: demand didn't disappear. Sourcing went underground.
Patients who previously obtained peptides through licensed compounding pharmacies — GMP oversight, batch traceability, sterility assurance, prescription oversight, API sourcing from FDA-registered facilities — turned to websites selling "research-use only" products from unverified overseas suppliers. DIY injection groups on Telegram. Raw peptide powder with no third-party testing.
The FDA has since documented the predictable fallout:
- USApeptide.com: Warning letter February 2025 for selling semaglutide and tirzepatide as "research chemicals" — products not approved for human use, sourced from unknown manufacturers
- Agebox iKids Growth Day Formula: FDA notification September 2025 — laboratory analysis found hidden ibutamoren in a product marketed for children
These are the documented cases. The ones nobody found aren't tracked, because nobody's looking at unregulated suppliers.
A policy justified by safety concerns created a categorically less safe market. The irony is thick enough to spread on toast.
The Peptides Being Reviewed — An Honest Evidence Accounting
BPC-157
Mechanism: 15-amino acid sequence from gastric protective protein. Modulates nitric oxide pathways, supports growth factor signaling, affects VEGF expression and extracellular matrix gene activity. Preclinical models show promotion of wound healing, gut protection, tendon and ligament repair, and protective effects across multiple injury models.
Evidence: 544 research articles published 1993-2024. Toxicology Research and Application, 2020 (PMID 32246197): zero acute toxicity in preclinical studies across rats, mice, rabbits, and dogs. Phase 1/2 human trials for ulcerative colitis conducted in Croatia, early 2000s. No completed Phase 3 trials.
Verdict: Strong preclinical safety signal. Limited clinical data. Extensively studied in animals. Almost no large-scale human trials.
Thymosin Alpha-1
Mechanism: Naturally occurring thymic peptide. Enhances T-cell function, NK cell activity, and dendritic cell maturation. Immunomodulatory.
Evidence: Approved in 30+ countries. Over 40 years of clinical use. Studied in hepatitis B/C, sepsis, and as an oncology adjuvant.
Verdict: The most clinically established peptide on the reclassification list by a significant margin. "Inadequate safety information" reads differently against 40 years of documented international use.
CJC-1295 and Ipamorelin
Mechanism: CJC-1295 is a GHRH analog. Ipamorelin is a selective ghrelin receptor agonist. Together: stimulated GH release without significant cortisol or prolactin elevation.
Evidence: Animal studies demonstrate increased GH and IGF-1. PCAC reviewed both in late 2024. FDA preliminary recommendation for ipamorelin: exclude from 503A bulks regulation.
Verdict: Extensive clinical observation, limited formal evidence. The gap between "limited data" and "unsafe" is substantial.
GHK-Cu (Injectable)
Mechanism: Copper-binding tripeptide. Stimulates collagen, elastin, and glycosaminoglycan synthesis. Upregulates approximately 4,000 genes related to tissue repair.
Evidence: Extensive in vitro and preclinical research. Decades of topical use — the evidence for topical GHK-Cu is well-established. Injectable form has significantly less human data.
Verdict: FDA's safety concerns are route-specific. That's a meaningful distinction most coverage misses.
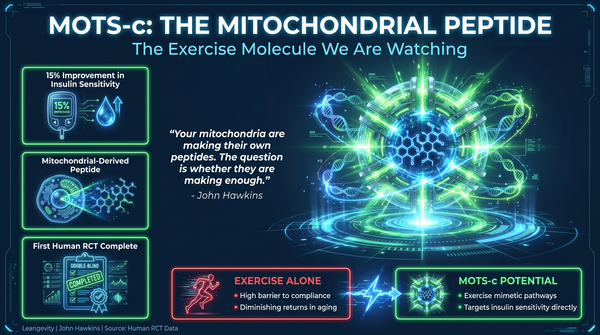
MOTS-c
Mechanism: Mitochondrial-derived peptide. Regulates metabolic signaling via AMPK pathway. Acts as an "exercise mimetic" in preclinical models. Discovered 2015.
Evidence: Preclinical mouse studies show metabolic improvements. Human data very early.
Verdict: Frontier science. Genuinely interesting mechanism. Insufficient human evidence to draw firm conclusions.
Your Actual Position Right Now
If you're on a compounded GLP-1: Review your sourcing. If your telehealth provider is claiming a shortage exception for semaglutide, that exception expired February 2025. Ask specifically: 503A pharmacy with batch testing? Patient-specific prescription? Or a compliance position that's narrowing by the week?
If you're interested in BPC-157 or other non-GLP-1 peptides: The regulatory window is opening. It's not open yet. PCAC reviews start July 2026 at earliest. The formal process takes 1-2+ years minimum.
If you're buying from research chemical websites: Products with zero quality control. No sterility testing. No batch verification. No prescription oversight. The contamination cases FDA has documented are the ones that got found.
The Meta-Point Most Coverage Misses
Most people get this wrong because they're either all-in or all-out on peptides. They treat Category 1 as a green light and Category 2 as evidence of danger. Both positions are wrong.
Category 1 is not FDA approval. Category 2 is not evidence of danger. These are regulatory designations reflecting the volume and quality of available evidence — not a binary verdict on safety.
Thymosin Alpha-1 has decades of documented international use. BPC-157 has extensive preclinical data. GHK-Cu has solid topical evidence. MOTS-c has an interesting mechanism with very early human data.
These are genuinely different evidence profiles. The regulatory reclassification process will sort them differently, one by one.
That's worth knowing before you treat all peptides as one category — either all dangerous or all promising.
And here's the consistent thread: regulated access is safer than unregulated access. The regulatory landscape is shifting in a specific direction. The people who benefit from whatever compounds become available — through regulated channels, with quality control, under professional oversight — will be the ones who built a metabolic foundation those tools can work on.
Peptides are tools. Tools work best on a solid system.
Build the foundation first. The tools are coming.
Leangevity provides metabolic health coaching, not medical treatment. Consult a licensed healthcare provider before starting, stopping, or changing any medication or supplement protocol.
Sources:
- FDA Warning Letters, March 3, 2026 (FDA.gov)
- FDA Policy Clarification on Compounded GLP-1s, April 1, 2026
- FDA Federal Register Notice, September 2023 — Category 2 Designation
- NYT, March 31, 2026 — "HHS Plans to Lift Restrictions on Some Compounded Peptides"
- WaPo, April 15, 2026 — "Federal Health Officials to Review Peptide Restrictions This Summer"
- JRE Episode 2461, February 27, 2026 (RFK Jr. appearance)
- Sikiric P et al., PMID 32246197, Toxicology Research and Application, 2020
- Venable LLP, March 2026 — Pharmacy Compounding Regulatory Analysis
- Rivkin Rounds, April 2026 — FDA Peptide Enforcement Landscape
Explore the Metabolic Mastery Protocol: https://leangevity.fit