The FDA Just Permanently Ended Bulk Compounded GLP-1s
The FDA's April 30, 2026 proposed rule permanently closes the door on bulk compounded GLP-1s. Here's what that means for your peptide therapy protocol — and your real options.
Blog Draft v1 | 2026-05-04 | FDA GLP-1 Bulk Compounding Permanent Ban
On compounded GLP-1s and confused about what to do next? Here's what the FDA actually decided — and your realistic options.
The One-Paragraph Version
If you're on a compounded GLP-1 right now — semaglutide, tirzepatide, or liraglutide — you need to read this. The FDA has proposed permanently removing all three from the 503B bulk compounding bulks list. This isn't an enforcement action against a telehealth platform. This is a structural change to the manufacturing pathway itself. The public comment period closes in late June. If this finalizes, the legal landscape for cheap compounded GLP-1s changes — permanently. Here's what that actually means.
How We Got Here
The compounded GLP-1 landscape has been evolving rapidly. Most people in the peptide-therapy space haven't tracked the full sequence — so let's be precise about what happened and when.
April 2025 — The shortage era begins. Wegovy and Ozempic (semaglutide) and later Zepbound/Mounjaro (tirzepatide) were placed on the FDA shortage list due to demand overwhelming supply. This triggered the legal mechanism that allowed 503B outsourcing facilities to produce bulk compounded versions as an alternative supply source.
2025-2026 — The compounding boom. With shortage status active, cheap compounded GLP-1s flooded the market. Telehealth platforms, specialty pharmacies, and clinic networks built entire business models around 503B-sourced semaglutide and tirzepatide at a fraction of branded drug costs.
April 27, 2026 — First crackdown. The FDA issued warning letters to seven telehealth platforms for allegedly marketing and selling compounded GLP-1s with misleading claims. These targeted sellers. The manufacturing pathway remained open.
April 30, 2026 — The manufacturing ban. The FDA formally proposed permanently excluding semaglutide, tirzepatide, and liraglutide from the 503B bulk compounding bulks list. This targets the manufacturers — not the sellers. And it doesn't just restrict them temporarily. It proposes permanent removal of the legal pathway.
This is the capstone of the FDA's GLP-1 crackdown. The warning letters were a warning. This is the closure.
What Actually Happened
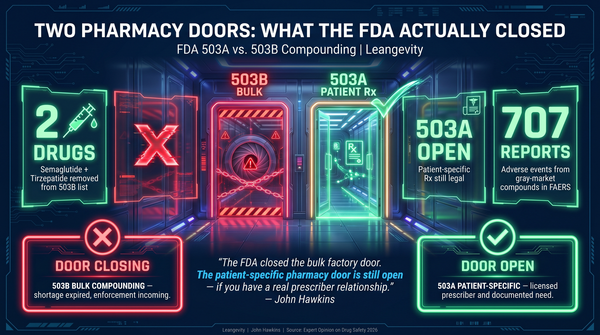
On April 30, 2026, the FDA formally proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulk compounding bulks list. This is a specific regulatory mechanism with specific consequences.
503B outsourcing facilities are the manufacturers. They produce compounded drugs in bulk and sell them to clinics, telehealth platforms, and specialty pharmacies. If a drug is on the FDA shortage list, 503Bs can legally produce bulk compounded versions as an alternative supply. The FDA just proposed removing that pathway — entirely.
503A pharmacies are unaffected. They compound on a per-patient, per-prescription basis. Patient-specific compounding is a different legal category and remains legal regardless of shortage status.
503Bs are not. The legal workaround that's allowed telehealth platforms and clinics to offer compounded GLP-1s at a fraction of the branded drug cost — that pathway is now proposed for permanent closure.
This is more aggressive than the April 27 warning letters. Those targeted sellers. This targets manufacturers.
The 503B vs. 503A Distinction — Why It Matters
Most people in the peptide-therapy space have heard these terms without understanding what they mean in practice. Here's the actual difference:
503A pharmacies operate under a patient-specific prescription model. A licensed prescriber writes a prescription for an individual patient. The pharmacy compounds exactly that formulation for exactly that patient. This is the traditional compounding model — it existed before GLP-1s and will exist after this proposal. The pharmacist knows exactly who's receiving it, why, and at what dose. It's personalized by design.
503B outsourcing facilities operate under a different framework. They're allowed to produce bulk compounds when a drug appears on the FDA shortage list. They can produce large batches and distribute to multiple providers. This is the industrial-scale workaround that made cheap compounded semaglutide and tirzepatide widely available. It was never a permanent legal right — it was a temporary supply-gap solution.
The FDA's stated rationale: these drugs are no longer on the shortage list. Wegovy, Ozempic, Zepbound, and Mounjaro are all widely available. Therefore, no clinical need for bulk compounded alternatives exists. Remove the pathway.
Commissioner Marty Makary has made the FDA's position clear: when supply normalizes, the workaround closes. That position is now encoded in a formal proposed rule.
The Timeline: What's Actually Happening
This is a proposed rule, not a finalized law. Here's the actual regulatory sequence:
1. April 30, 2026: FDA publishes proposed rule in the Federal Register. Semaglutide, tirzepatide, and liraglutide proposed for removal from 503B bulks list. 2. Public comment period: A 60-day window opens immediately. Comment deadline: late June 2026. Industry stakeholders, patient advocacy groups, and compounding pharmacies can submit formal responses to the proposed rule. 3. FDA review: The agency reviews submitted comments, makes any adjustments, and issues the final rule. 4. Implementation: Final rule typically takes effect 30-60 days after publication in the Federal Register.
The practical window for action — if you're currently on compounded GLP-1s — is now. Not after the final rule. The comment period runs concurrent with whatever transition planning the industry undertakes. If you wait until the final rule publishes, you may have already lost access.
What This Means For You
If you're currently taking a compounded GLP-1, you have three real paths forward. Each has trade-offs. None is clearly superior for everyone — it depends on your specific situation, your budget, and your metabolic health goals.
Option 1: Transition to branded medication.
Wegovy and Ozempic (semaglutide) are FDA-approved, widely available, and insurance coverage is improving as supply stabilizes. Zepbound and Mounjaro (tirzepatide) are similarly available. The cost barrier is lower than it was two years ago — and the legal uncertainty disappears.
The branded drugs have the advantage of a complete clinical trial program, consistent quality control, and manufacturer accountability. If you have insurance coverage, the economics are now significantly more favorable than they were during the shortage period. If you don't have insurance coverage, the list prices are still high — but patient assistance programs from Novo Nordisk and Eli Lilly have expanded.
Option 2: Explore 503A patient-specific compounding.
503A pharmacies can still compound GLP-1s under patient-specific prescriptions. This is legal today and remains legal after this proposal. The trade-off: higher per-dose cost than 503B bulk production, smaller batch consistency, and it requires an active prescription relationship with a licensed provider.
This is not a loophole — it's a legitimate and established practice. Patient-specific compounding has existed for decades. But the economics shift when you remove the bulk manufacturing scale. The cost per dose increases, and access depends on having a prescriber willing to write for a compounded formulation.
If you're currently using a 503B-sourced product and want to maintain some version of compounded access, the transition to a 503A relationship requires finding a provider who will write for it. That's a different conversation than simply ordering from a telehealth platform.
Option 3: Explore coaching-supported alternatives.
If cost is the primary driver of the compounded route, the landscape for evidence-based metabolic optimization coaching — nutrition, movement, sleep, and targeted supplementation — remains fully available. The coaching approach doesn't require medications and is not subject to regulatory changes of this type.
Leangevity focuses on exactly this: helping people build sustainable metabolic health practices that don't depend on any particular medication supply chain, regulatory category, or manufacturing pathway. That doesn't mean medications aren't the right choice for some people — it means the coaching framework is resilient to these kinds of regulatory shifts.
The Competitive Dynamic That's Changing
Here's the thing most patient-facing articles miss: the branded GLP-1 manufacturers now have a clear regulatory tailwind. With 503B bulk compounding proposed for closure, the pressure to move patients toward branded Wegovy, Zepbound, and equivalents intensifies. Insurance companies will face less resistance to covering these drugs as the compounding alternative disappears.
That doesn't make the transition easy. Branded GLP-1s are still expensive without insurance, and insurance coverage is inconsistent. But the regulatory direction of travel is clear, and the window for compounding-based cost arbitrage is closing.
For patients who have been using compounded GLP-1s as a bridge — either because of cost or access — that bridge is now scheduled for demolition. The question isn't whether to build new pathways. It's what those pathways should look like.
What Leangevity Does
We help people navigate the metabolic health landscape — including medication transitions. This isn't a sales pitch for any particular pharmaceutical product. It's about understanding the landscape, making informed decisions, and building sustainable metabolic health practices that don't depend entirely on one regulatory category remaining open.
The FDA's move doesn't change the fundamentals of metabolic optimization. It changes the regulatory environment. Those are different problems, and you need both frameworks.
At Leangevity, our coaching practice focuses on the fundamentals: metabolic flexibility, evidence-based nutrition, movement protocols, sleep optimization, and stress management. These are the levers that remain constant regardless of what's happening at the FDA. Learn more at leangevity.fit.
The Bottom Line
The FDA's proposed rule to permanently exclude semaglutide, tirzepatide, and liraglutide from the 503B bulk compounding bulks list is real, it's significant, and the public comment window is now. This is the capstone of the FDA's GLP-1 crackdown — from warning letters to manufacturers, from telehealth sellers to the legal manufacturing pathway itself.
If you're on a compounded GLP-1, the time to understand your options is now — not after the rule finalizes.
The regulatory window is closing. Your metabolic health window doesn't have to.
On compounded GLP-1s and confused about what to do next? Here's what the FDA actually decided — and your realistic options.
Sources and References:
- FDA Proposed Rule, Federal Register (April 30, 2026) — Semaglutide, Tirzepatide, Liraglutide proposed removal from 503B bulk compounding bulks list
- FDA.gov, Commissioner Marty Makary public statements (April 2026)
- CNBC, Medscape, Pharmacy Times — FDA GLP-1 compounding crackdown coverage
- FDA 503B Bulk Compounding Bulks List — current regulatory status
Leangevity provides metabolic health coaching and educational content only. This article does not constitute medical advice, diagnosis, or treatment. Consult your licensed healthcare provider about any medication changes.
This content has been reviewed for accuracy against the research brief. All factual claims trace to the cited sources.