GLP-1s Are Not Being Banned. The Shortcut Is Being Closed.
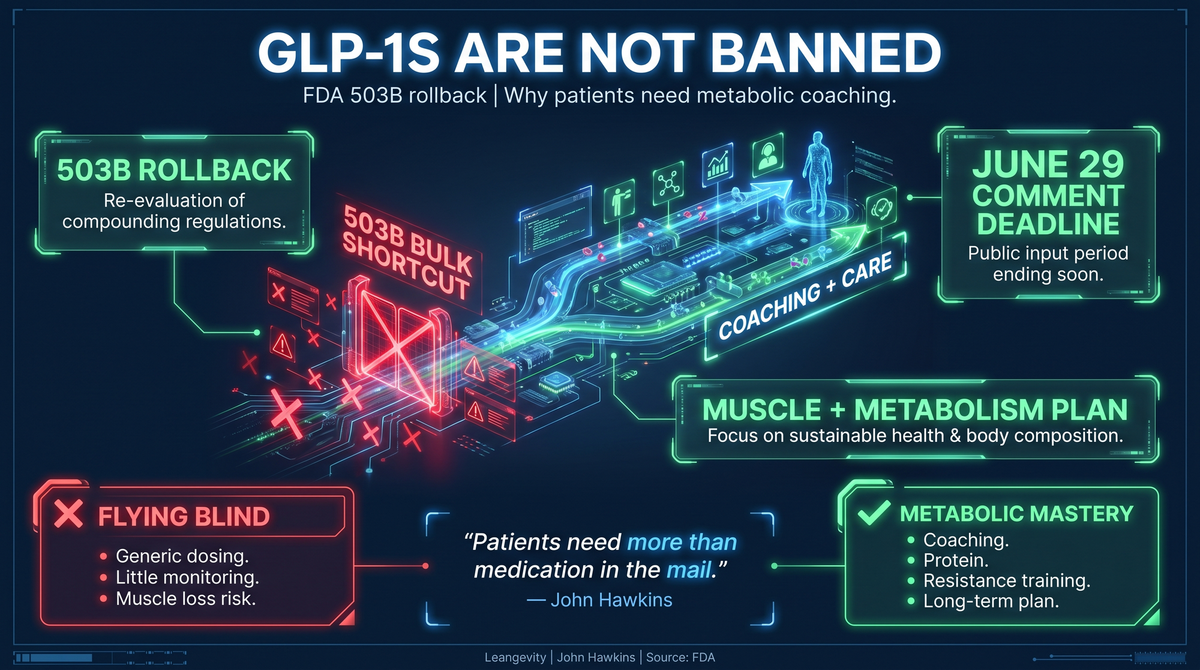
GLP-1s are not being banned. The FDA is rolling back the 503B bulk-manufacturing shortcut, and patients need more than medication in the mail.
The FDA is not banning GLP-1 medications.
Not surprisingly, the internet got it wrong. Here is what’s really happening.
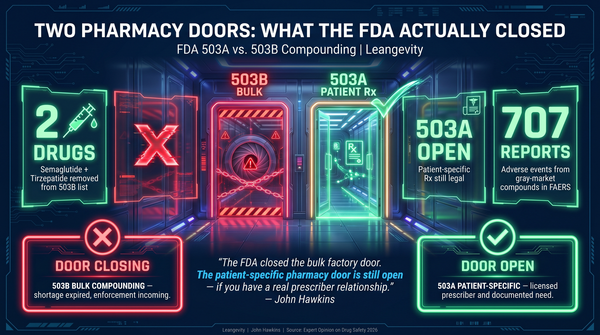
On April 30, 2026, the FDA proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list. That sounds technical because it is technical. The simple version is this: large outsourcing pharmacies would no longer have the same pathway to bulk-manufacture these GLP-1 drugs from raw bulk substances.
That is not a blanket ban on GLP-1s. It is not even a blanket ban on every form of compounding. It is a rollback of the high-volume 503B shortcut that grew during the shortage era.
And frankly, that shortcut needed to close.
The shortage excuse is going away
The legal and practical reason for much of the compounded GLP-1 boom was shortage. Demand exploded. Brand-name supply lagged. Patients wanted access. Telehealth companies saw a market. Compounding pharmacies had a pathway.
That pathway made sense as an emergency pressure valve.
But emergency pressure valves are not supposed to become the business model.
The FDA’s position is direct: if FDA-approved commercial products are available, there is no clinical need for 503B outsourcing facilities to compound these same drugs from bulk substances. The agency is taking public comment through June 29, 2026, so the rule is proposed, not final. But the direction is clear.
Name-brand manufacturers have scaled production. The market no longer looks like it did at the peak of the shortage. So the rules are functioning as intended.
That will make a lot of people angry. Especially the companies that built huge businesses around the shortage.
This is bad for the mail-order GLP-1 machine
The big losers are not patients who need help losing weight.
The big losers are the large, high-volume telehealth operators that turned GLP-1 access into an ecommerce funnel.
You know the model. Online intake. Fast approval. Medication shipped to the house. Same general schedule. Little monitoring. Minimal coaching. Refill pipeline.
That model scales. It also leaves patients flying blind.
GLP-1 medications are powerful. They change hunger, appetite, gastric emptying, food intake, and body-weight regulation. They can help the right patient at the right time. But powerful tools need supervision.
When patients are given generic schedules with poor follow-up, predictable problems show up.
Nausea gets ignored until eating becomes miserable. Constipation becomes normal. Protein intake collapses. Muscle loss accelerates. Patients under-eat, lose scale weight, then wonder why they feel weaker and flatter. Dosing mistakes become more likely. Side effects become harder to interpret.
This is not a medication problem by itself. It is a care-model problem.
The FAERS pharmacovigilance signal on compounded GLP-1 products adds another layer. A 2026 analysis identified compounded-product adverse-event reports, including medication errors and product-quality concerns. That does not prove every compounded product is unsafe. It does prove that high-volume access without strong guardrails is not a trivial issue. PMID 40285721.
The brand-name system is not innocent
Here is where the other side gets uncomfortable.
The branded GLP-1 world often makes the same mistake in a cleaner package.
A patient gets the prescription. The pharmacy fills it. Then the follow-up happens three months later when the refill is due.
That is not a metabolic plan. That is a transaction.
The drug is doing part of the work. Appetite drops. Calories drop. Scale weight moves. Everyone feels like the plan is working.
But what is happening under the hood?
Is the patient eating enough protein? Are they lifting? Are they preserving muscle? Are they sleeping? Are they correcting insulin resistance? Are they rebuilding food structure? Are they learning how to eat when hunger comes back? Are they building the maintenance plan before the dose changes?
Most patients are not.
They are just smaller versions of the same metabolically broken system.
That is how weight comes back. That is how muscle gets lost. That is how people become dependent on the medication because nothing else changed.
The drug made the work easier. It did not replace the work.
The real problem is flying blind
The argument should not be “compounders good, FDA bad.”
It should not be “brand-name drugs good, compounders bad.”
The real problem is flying blind.
Patients struggling with obesity and metabolic dysfunction do not need another shortcut sold as a solution. They need a guide.
They need someone watching the obvious failure points:
- Protein falling too low
- Strength training never starting
- Constipation getting normalized
- Nausea being treated like a badge of honor
- Calories dropping so low that muscle becomes the fuel source
- No plan for what happens when the medication changes
- No metabolic education beyond “eat less”
That is not care. That is a countdown to regain.
The medication may open the window. Coaching teaches the patient what to do while the window is open.
503A is not the same as 503B
This distinction matters.
The FDA proposal is about 503B outsourcing facilities and the bulk-substance pathway. It does not mean every compounded GLP-1 is gone. It does not mean 503A patient-specific compounding is banned.
Reputable 503A providers may still operate under patient-specific rules when clinically appropriate. That is a different model.
The key distinction is not just a pharmacy acronym. It is the care structure around the patient.
High-volume bulk access asks, “Can we ship this at scale?”
Patient-specific care asks, “What does this person need, how are they responding, and who is watching?”
That is the better question.
Leangevity is not here to tell people where to source medication. That is not our role. Medication decisions belong with licensed medical providers.
Our role is the work most patients are not getting anywhere else.
GLP-1s are a shortcut, not the destination
There is nothing wrong with using a shortcut when the road is broken.
Most people with serious weight problems are not lazy. Their metabolism has been trained in the wrong direction for years. Bad nutrition advice. Hyper-palatable food. Poor sleep. No muscle signal. Insulin resistance. A nervous system running on stress. A body that cannot easily access stored fuel.
A GLP-1 can lower the noise.
It can make hunger manageable. It can create space. It can help a patient stop fighting biology every hour of the day.
That is valuable.
But the quiet is temporary if you do not use it correctly.
While the medication is making the work easier, the patient has to build the system they should have had all along: protein, muscle, food structure, metabolic flexibility, sleep, labs, habits, and a maintenance plan.
That is metabolic mastery.
Not a slogan. A sequence.
What patients should do now
If you are using a GLP-1, do not panic. GLP-1s are not being banned.
But do not ignore the signal either.
The shortage-era market is changing. The cheap high-volume shortcut is getting squeezed. If your entire plan depends on easy access, no coaching, and a refill shipment, your plan is fragile.
Ask better questions.
Who is monitoring your response? Who is watching side effects? Who is helping you protect muscle? Who is tracking protein? Who is helping you build the eating pattern you will need later? Who is teaching you how to keep fat burning when the medication is reduced or stopped?
If the answer is nobody, that is the problem.
This is why Leangevity exists.
Regardless of where the medication comes from, the patient still needs guidance. Better nutrition. Muscle preservation. Energy restoration. Metabolic education. A plan that survives beyond the prescription.
The goal is not to be on a drug forever with less appetite and less muscle.
The goal is to burn fat, maintain muscle, increase energy, and live a lean, healthy life longer.
That requires more than a medication in the mail.
It requires a system.
The bottom line
The FDA is not ending weight-loss medicine.
It is closing a high-volume shortcut that became less defensible once supply improved.
That is bad for companies that treated shortage-era GLP-1 access like a growth channel. It may be good for patients if it forces the market back toward individualized care.
But only if patients understand the real lesson.
The drug can make the work easier. It cannot replace the work.
Read the full Leangevity breakdown and coaching framework here: https://blog.leangevity.fit/glp-1-503b-compounding-rollback/
Sources:
- FDA April 30, 2026 announcement: https://www.fda.gov/news-events/press-announcements/fda-proposes-exclude-semaglutide-tirzepatide-and-liraglutide-503b-bulks-list
- FAERS compounded GLP-1 pharmacovigilance signal: PMID 40285721
Medical disclaimer: This content is for education and coaching only. It does not constitute medical advice, diagnosis, treatment, prescribing guidance, or pharmacy recommendation. Consult your licensed healthcare provider about medication decisions.
Two plain-English definitions
Metabolic dysfunction means the body has trouble using fuel. The patient has stored energy, but the system cannot use it well. Insulin resistance means insulin has to shout louder to do the same job. When that signal stays high, fat burning stays harder.
That is why coaching matters. The medication may reduce hunger, but the patient still has to rebuild the fuel system. Food choices, protein, muscle, sleep, and daily structure are not side notes. They are the plan that makes the result last.