GLP-1 Drugs Are Entering the Alcohol Conversation
A Lancet RCT suggests semaglutide may affect heavy drinking days in adults with alcohol use disorder and obesity—but the story is biology, not hype.
GLP-1 Drugs Are Entering the Alcohol Conversation
The most interesting GLP-1 story right now may not be weight loss.
A 2026 randomized trial in The Lancet suggests semaglutide may reduce heavy drinking days in treatment-seeking adults with moderate-to-severe alcohol use disorder and obesity. That does not mean semaglutide cures alcohol use disorder. It does not mean Leangevity treats alcohol use disorder. It means the GLP-1 category just walked into a room most people did not expect it to enter.
Medicine has a habit of discovering that one system talks to another system. Then everyone acts surprised. The body, apparently, did not read our clinic org chart.
Obesity was the first chapter. It may not be the whole book.
Most people still think about GLP-1 drugs through one lens: appetite and weight loss.
That lens is not wrong. It is just incomplete.
The new trial is useful because it does not ask whether semaglutide helps people lose weight. It asks a narrower and more clinically interesting question: in adults seeking treatment for alcohol use disorder who also have obesity, does semaglutide reduce heavy drinking days when added to standard cognitive behavioral therapy?
That is a different question.
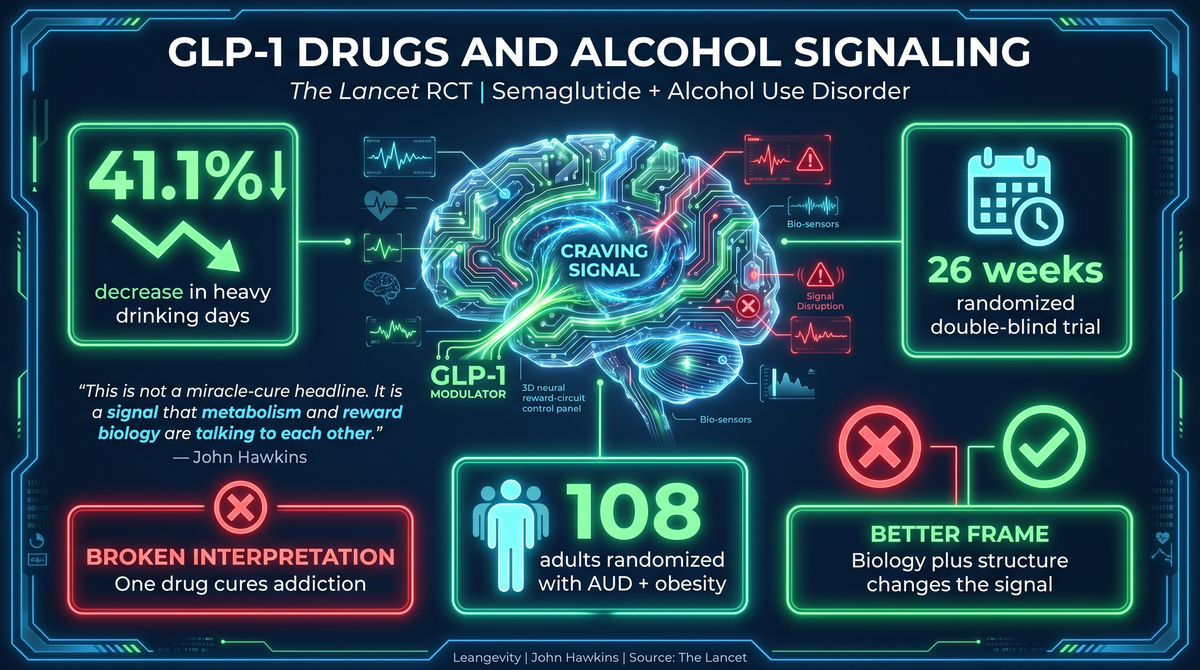
The trial was randomized. It was double-blind. It was placebo-controlled. It ran for 26 weeks at a single center. It included 108 randomized participants: 54 assigned to semaglutide and 54 assigned to placebo. Both groups also received standard CBT. Eighty-eight participants completed the intervention.
That is not a headline. That is a study design.
And study design matters, because this topic is a magnet for nonsense. The internet will turn one trial into a miracle by lunchtime. Then someone will sell a protocol by dinner. Efficient, if nothing else.
The data deserves a cleaner reading.
The trial did not test “willpower.” It tested biology plus structure.
Alcohol use disorder is not a character flaw. Neither is obesity.
Both involve systems that regulate drive, reward, appetite, impulse, and feedback. That does not remove personal responsibility. It puts responsibility in the right place: inside a system that can be measured and managed.
In the Lancet trial, participants were treatment-seeking adults with moderate-to-severe alcohol use disorder and comorbid obesity. They were not casual drinkers trying to “cut back for summer.” They were a clinically defined population.
Both groups received standard CBT. One group also received semaglutide. The other received placebo.
That matters because the study did not compare medication against nothing. It compared semaglutide plus behavioral treatment against placebo plus behavioral treatment.
This is the right frame.
Behavioral structure still matters. Coaching still matters. Medical care still matters. The question is whether changing metabolic signaling may shift the feedback loop enough to improve outcomes.
The answer, in this trial, was yes for the primary outcome.
Heavy drinking days dropped more with semaglutide.
The primary outcome was heavy drinking days after 26 weeks.
Here is the result from Kruse Klausen et al., published in The Lancet in 2026, PMID 42070571:
- Semaglutide group: heavy drinking days decreased by 41.1 percentage points from baseline.
- Placebo group: heavy drinking days decreased by 26.4 percentage points from baseline.
- Estimated treatment difference: -13.7 percentage points.
- 95% confidence interval: -22.0 to -5.4.
- p-value: 0.0015.
That is the signal.
Not “cure.” Not “replacement for addiction care.” Not “take a GLP-1 and your drinking problem disappears.”
A 13.7 percentage-point treatment difference over 26 weeks is worth paying attention to. It is also not permission to turn a clinical trial into a social media prescription pad.
The math matters. So do the boundaries.
The control group improved too. Do not miss that.
The placebo plus CBT group also improved substantially.
Heavy drinking days decreased by 26.4 percentage points from baseline in the placebo group. That is not trivial. It tells you the behavioral treatment environment mattered.
This is where people usually get the interpretation wrong.
They see the drug effect and forget the context. The study did not isolate semaglutide in a vacuum. It tested semaglutide in addition to standard CBT in a treatment-seeking population.
In plain English: the system improved when the system was treated.
The semaglutide group improved more. But both groups were inside a structured intervention.
This is exactly how Leangevity thinks about metabolic health, with one important compliance boundary: Leangevity provides coaching for metabolic health. It does not diagnose, treat, or manage alcohol use disorder. Medication questions belong with a licensed clinician. Different lane. Same human body.
Blurring those lanes is how people get into trouble.
A signal is not a protocol.
This trial gives us a signal.
It does not give the public a treatment protocol.
The study used once-weekly semaglutide in a clinical trial setting with standard CBT. I am not giving dosing guidance here. I am not telling anyone to start, stop, combine, or repurpose a medication. That belongs to a licensed clinician who knows the patient, the diagnosis, the medication list, the risk profile, and the rest of the boring details that keep medicine from becoming roulette.
The point is not “go ask for semaglutide for drinking.”
The point is that GLP-1 drugs may be forcing medicine to think more broadly about metabolic signaling and behavior.
For years, weight loss was treated like a willpower contest. Eat less. Move more. Try harder. Then GLP-1 drugs made it obvious that appetite is regulated by biology, not moral fiber.
Now alcohol research may be following a similar pattern.
Not identical. Not proven as a broad use case. But similar enough to watch closely.
Safety still counts. The gut had opinions.
The trial reported transient, generally mild-to-moderate gastrointestinal adverse effects, more frequent in the semaglutide group.
That is not a throwaway line.
GLP-1 drugs can be effective tools in the right clinical setting. They can also be poorly tolerated. The gastrointestinal system tends to send memos in all caps.
This is another reason the “anti-addiction medication” headline needs adult supervision.
A drug effect is only one part of the decision. Tolerability matters. Patient selection matters. Clinical monitoring matters. The underlying diagnosis matters. The presence of obesity in this trial matters. The fact that participants were treatment-seeking matters. The CBT context matters.
Remove those details and you are no longer discussing the study. You are discussing vibes wearing a lab coat.
We do not do that here.
The Leangevity takeaway is not “medicate behavior.”
The Leangevity takeaway is simpler.
Behavior is downstream of physiology more often than people want to admit.
That does not mean physiology excuses every behavior. It means the feedback loop matters. Hunger, craving, impulse, energy, weight, and metabolic dysfunction do not live in separate filing cabinets.
After treating over 3,000 patients, I have seen this pattern repeatedly: people blame themselves for a system failure. They think they are weak because they cannot out-discipline a body that is misfiring.
Then the right levers change. Hunger changes. Energy changes. Compliance changes. The person did not suddenly become virtuous. The system stopped screaming.
That is why this trial is worth tracking.
It suggests GLP-1 therapy may have effects that extend beyond the scale in a defined clinical population. It also reminds us that clinical tools work best inside a larger structure: medical oversight, behavior support, nutrition, sleep, resistance training, and honest monitoring.
No glitter. No fairy dust. Just systems.
Where Leangevity fits — and where it does not.
Leangevity is a metabolic health coaching platform. The work is education, behavior architecture, nutrition structure, training habits, and metabolic strategy.
Leangevity does not treat alcohol use disorder.
Medication decisions belong with licensed clinical care. Leangevity stays in metabolic-health education and coaching. If those sound interchangeable, the compliance officer just developed a twitch.
For someone interested in GLP-1 therapy, the right question is not “Can this drug fix everything?”
The better question is:
- What is the medical indication?
- What is the metabolic context?
- What support structure is in place?
- What outcomes are being measured?
- Who is monitoring safety?
That is how adults use powerful tools.
If you want coaching around metabolic health, nutrition structure, body composition, and behavior systems, start at leangevity.fit. If your question is clinical, diagnostic, or medication-related, bring it to your licensed clinician.
Different lanes. Cleaner outcomes.
What to watch next.
This was one randomized, double-blind, placebo-controlled trial with 108 randomized participants and 88 completers.
It was enough to create a real signal. It was not enough to declare the case closed.
The next useful questions are straightforward:
- Can the finding be replicated?
- Does it apply outside adults with alcohol use disorder and obesity?
- How durable is the effect after intervention ends?
- Which patients are most likely to respond?
- How should tolerability and safety be managed in real-world care?
Those questions matter because medicine tends to overcorrect.
First it ignores a signal. Then it worships it. Then it sells it. Then it spends five years cleaning up the mess.
A better approach is to track the evidence, respect the boundaries, and avoid pretending one trial answers every question.
Bottom line.
A 2026 Lancet randomized trial found that semaglutide plus CBT reduced heavy drinking days more than placebo plus CBT in treatment-seeking adults with moderate-to-severe alcohol use disorder and obesity.
The estimated treatment difference was -13.7 percentage points after 26 weeks.
That is clinically interesting.
It is not a cure claim. It is not a Leangevity treatment recommendation. It is not dosing advice. It is a strong enough signal to watch closely and a good reminder that metabolism, appetite, behavior, and feedback loops are more connected than the old model allowed.
Obesity was the first public GLP-1 story.
It may not be the last.
Sources:
- Kruse Klausen et al. Semaglutide alcohol use disorder randomized controlled trial. The Lancet. 2026. PMID: 42070571.
Leangevity provides metabolic health coaching, not medical treatment. Nothing in this article constitutes medical advice, diagnosis, or treatment. Leangevity does not diagnose, treat, or manage alcohol use disorder. Always consult your licensed clinician before making any changes to your medication plan.
Learn more about Leangevity at leangevity.fit.