The GLP-1 Exit Strategy: What Happens After You Stop?
50-67% of weight returns after stopping GLP-1s. Here's the clinical data on weight regain, muscle loss, and the trial testing the exit.
Here's what's actually happening, and it's the question that most GLP-1 patients should be asking but aren't.
ClinicalTrials.gov lists trial NCT06605703, which specifically compares the effectiveness of weight management options after patients discontinue GLP-1 receptor agonist therapy. The trial addresses the question that the pharmaceutical trials deliberately avoided: what happens when you stop?
Because we already know what happens. The data is clear, and it's not favorable for long-term sustainability.
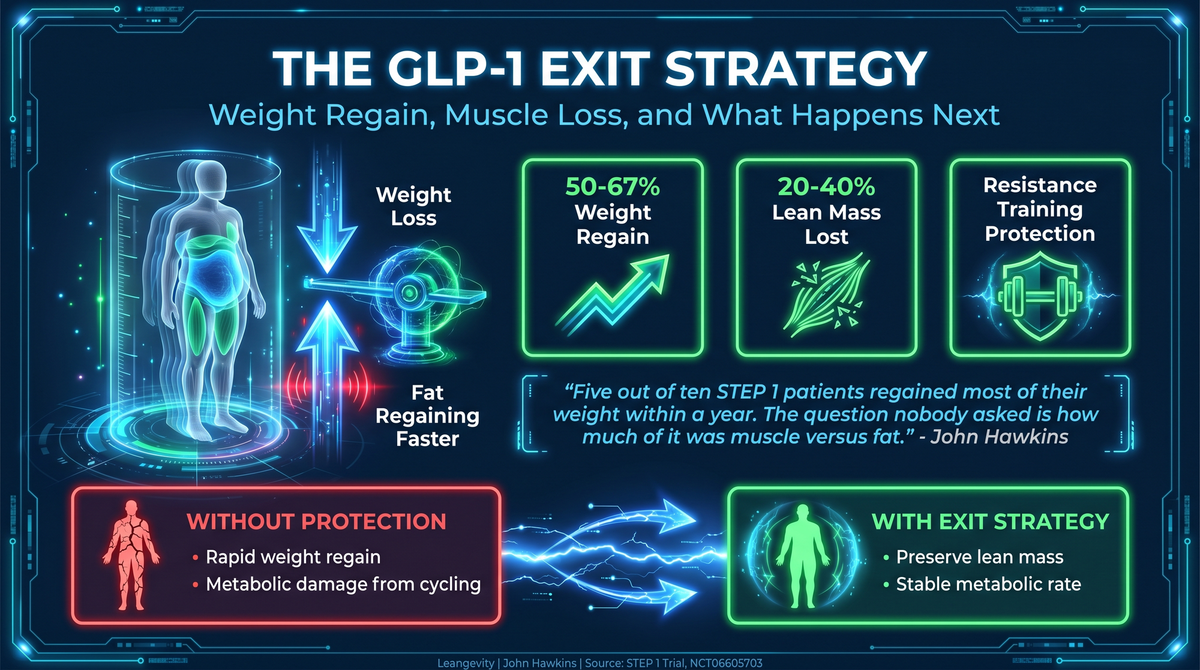
What the Existing Discontinuation Data Shows
The STEP 1 extension trial — the longest follow-up on semaglutide 2.4mg in the obesity population — demonstrated that patients who discontinued the drug regained approximately 50-67% of their lost weight within one to two years. The mean weight loss during active treatment was about 15%. The regain trajectory was rapid and consistent, with most patients returning to near-baseline weight within two years of discontinuation.
This isn't a patient adherence problem. This isn't behavioral failure. This is the pharmacology working exactly as designed. GLP-1 receptor agonists reduce appetite, delay gastric emptying, and modulate central satiety signaling. When the drug stops, those effects stop. The body's homeostatic response — increased caloric intake, metabolic adaptation, preferential fat regain — restores the pre-treatment equilibrium.
The clinical significance of this finding cannot be overstated. Weight cycling — losing weight, regaining it, losing it again — is associated with increased cardiovascular risk, reduced insulin sensitivity, increased inflammatory burden, and accelerated sarcopenia. Each cycle reduces muscle mass relative to fat mass. The body becomes progressively more metabolically compromised even as total weight returns to baseline.
This is the hidden cost of the pharmacological approach that isn't discussed in any advertisement.
The Muscle Loss Problem Nobody Addresses
Here's the part of the GLP-1 conversation most coverage skips entirely.
GLP-1 agonists don't just cause you to lose fat. You lose lean body mass at the same time. The STEP program data indicates that approximately 20-40% of total weight lost on semaglutide was lean mass — muscle, bone, and organ tissue. For a patient losing 30 pounds, that could mean 6-12 pounds of lean tissue.
This is a problem because lean mass is the single strongest predictor of long-term health outcomes in aging populations. Sarcopenia — age-related loss of muscle mass and function — affects 27% of older adults (PMID: 39813010). It's a stronger predictor of mortality and functional decline than BMI. And muscle preservation is the number one longevity intervention after age 40.
Mitochondrial dysfunction in muscle tissue accelerates with age (PMID: 23845738). Resistance training provides cross-education benefits for stroke recovery (PMID: 39455849). These are the same mechanisms that determine whether GLP-1-induced weight loss is healthy weight loss or metabolically harmful weight loss.
When a patient stops a GLP-1 agonist and regains weight, the regained mass is approximately 90% fat. The muscle they lost doesn't come back with the same speed. Over multiple weight loss-regain cycles, the body composition progressively shifts toward lower muscle-to-fat ratios — even at stable total body weight.
A patient who weighs 200 pounds before treatment, loses to 170 on the drug, and regains to 200 after discontinuation is not the same 200 pounds. The composition has shifted. The muscle-to-fat ratio is lower. The insulin resistance is likely worse than before treatment. The inflammatory burden is elevated.
This is the biological reality of weight cycling. It's the unaddressed consequence in every GLP-1 marketing campaign.
What the Exit Strategy Trial Is Testing
The NCT06605703 trial compares weight management options post-GLP-1. The specific interventions being compared may include:
- Structured nutritional intervention
- Resistance training protocols
- Combination behavioral and metabolic support
- Reduced-dose GLP-1 maintenance
- Alternative pharmacological agents
The trial's design matters because currently, the standard clinical advice after GLP-1 discontinuation is vague: "maintain healthy lifestyle changes." This is advice given to patients whose biology is actively driving them to regain weight. It's like telling someone to hold an umbrella in a hurricane.
What we need — what this trial aims to provide — is evidence-based protocols for the transition period. Specific nutritional parameters. Definitive resistance training prescriptions. Potentially maintenance medication strategies that minimize metabolic disruption while reducing drug exposure.
What Functional Medicine Currently Recommends
The data supporting specific interventions during GLP-1 transition is limited, but the mechanism-based approach is clear:
Resistance Training — Non-Negotiable
The protein meta-analysis (PMID: 39813010) evaluated plant versus animal protein for muscle health across 43 randomized controlled trials. The standardized mean differences demonstrate that protein quality matters for sarcopenia prevention. Patients transitioning off GLP-1 should be consuming 1.6-2.2 grams of protein per kilogram of body weight daily, distributed across 3-4 meals, combined with resistance training at least 3 times per week.
The stroke recovery study (PMID: 39455849) demonstrated that unilateral resistance training produced measurable improvements in hand grip strength, muscle thickness, and upper limb functionality in just 4 weeks. This isn't just for athletic populations — it's a fundamental metabolic intervention for anyone at risk of accelerated muscle loss.
Insulin Sensitization
The chronotype study (PMID: 35429387) demonstrated that metabolic syndrome patients with late chronotypes showed reduced peripheral insulin sensitivity, altered TCA cycle intermediate concentrations, and impaired beta-oxidation compared to early chronotypes on euglycemic clamp testing. Insulin sensitivity isn't a fixed trait — it's modifiable through sleep alignment, meal timing, and substrate management.
For patients coming off GLP-1, the drug has been artificially maintaining insulin levels at a lower set point. When the drug stops, the body's endogenous insulin response reactivates — and if insulin sensitivity hasn't been built during the treatment period, the rebound is more severe.
The exit strategy should include a structured transition off the GLP-1 effect — gradually reducing the dose while simultaneously implementing:
- Time-restricted eating aligned with circadian biology
- Resistance training to maintain and rebuild lean mass
- Adequate protein intake to support muscle protein synthesis
- Sleep optimization to support growth hormone release and cortisol normalization
Metabolic Flexibility Training
The TCA cycle intermediate data from the chronotype study (PMID: 35429387) provides a mechanistic window into metabolic flexibility — the body's ability to switch between fuel sources (glucose and fatty acids) based on availability. Late chronotype patients with metabolic syndrome showed impaired fuel switching.
GLP-1 patients who've been in a pharmacologically-induced low-calorie state may have reduced metabolic flexibility — their bodies have been running on restricted substrate for months or years. The exit strategy should include gradual caloric re-normalization combined with structured exercise that trains fuel-switching capacity.
The Drug Maintenance Question
Here's the debate the GLP-1 community isn't having: is indefinite GLP-1 use actually the right answer?
The cardiovascular data says yes. The SELECT trial showed that semaglutide 2.4mg reduced major adverse cardiovascular events in adults with obesity and cardiovascular disease over approximately three years of treatment. If GLP-1 provides cardioprotection independent of weight loss — and the data suggests it does — then permanent use might be clinically justified.
The metabolic data says it depends. Weight cycling is harmful. But permanent pharmacological appetite suppression is a metabolic experiment nobody has completed yet. The longest GLP-1 obesity trial follow-up is approximately five years. We're looking at patients who might use these drugs for decades.
The muscle mass data is a significant concern. Permanent GLP-1 use means permanent lean mass reduction — which accelerates with age. The sarcopenia trajectory on lifelong GLP-1 therapy is not known, because the trial duration hasn't been long enough to capture it.
A Functional Medicine Specialist's approach: consider GLP-1 as a bridge therapy, not a destination. Use the drug to achieve metabolic improvements — better insulin sensitivity, reduced inflammation, improved cardiovascular markers — then transition to lifestyle-based maintenance. If cardiovascular risk factors remain elevated, reconsider the risk-benefit ratio.
The Timeline for Transition
The trial NCT06605703 will provide structured data on the optimal transition approach. Until then, the evidence-based framework is:
1. Begin resistance training during GLP-1 treatment — don't wait until discontinuation. Build lean mass while the drug facilitates reduced caloric intake and lower training recovery barriers.
2. Implement protein-optimized nutrition — 1.6-2.2 g/kg daily with adequate leucine per meal for muscle protein synthesis.
3. Gradually taper GLP-1 dose — don't stop cold. A stepwise reduction over 8-16 weeks allows the body's endogenous appetite regulation to recalibrate.
4. Monitor body composition, not just weight — DEXA scans or bioelectrical impedance at baseline, during treatment, and during transition. Track lean mass retention, not just total weight.
5. Evaluate metabolic markers during transition — fasting insulin, HOMA-IR, HbA1c, inflammatory markers. The goal is metabolic stability, not just weight maintenance.
This is the exit strategy the pharmaceutical trials didn't study and the clinical guidelines haven't defined. It's the gap between "the drug works" and "you can stop the drug."
Filling that gap is what separates effective functional medicine from prescription management.
Explore the metabolic optimization protocols and transition support at leangevity.fit
P.S. — The patients who transition successfully off GLP-1 aren't the ones with the most willpower. They're the ones who used the treatment period to build real metabolic infrastructure. Better insulin sensitivity. More muscle mass. Improved mitochondrial efficiency. The drug provides the metabolic room to build these. If you don't build them during treatment, there's nothing to sustain the weight loss when the drug stops.