MOTS-c and the July 23 Decision That Could End Compounding Access
MOTS-c is the only peptide with two human trials. One proved it worked — then the company dissolved. The second is running. July 23, the FDA decides compounding access.
The Paradox: A Peptide With Actual Human Data — And No One To Sell It
Most peptides in the longevity space survive on animal data, extrapolated mechanisms, and enthusiastic anecdotes. MOTS-c is different. There are two human trials. Not one. Two. That alone puts it in a different category than anything else being compounded today.
But here's what most people don't know: the company that ran the first trial no longer exists.
What MOTS-c Actually Is
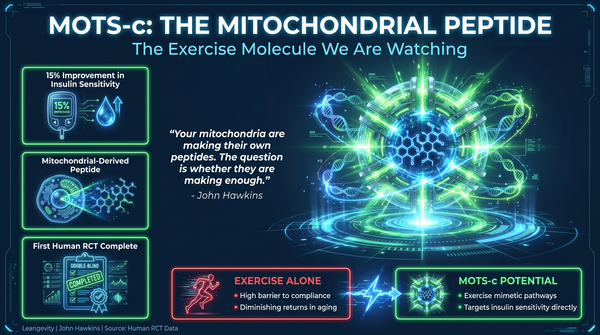
MOTS-c stands for Mitochondrial Open Reading Frame of the 12S rRNA Type-C. It is one of a class of mitochondrial-derived peptides — short bioactive proteins encoded in mitochondrial DNA that act as signaling molecules between the mitochondria and the rest of the cell.
MOTS-c was first characterized in 2015 by Lee et al., published in Cell Metabolism (PMID: 25738459). The original paper demonstrated that MOTS-c acts as an exercise mimetic, improving insulin sensitivity and reducing body weight in diet-induced obese mice through activation of the AMPK pathway. Subsequent work by Kim et al. (PMID: 31293078) showed that MOTS-c modulates sphingolipid and monoacylglycerol metabolism — pathways directly implicated in insulin resistance and fatty liver disease.
In human biomarker studies, circulating MOTS-c levels are lower in obese individuals and positively associated with insulin sensitivity (PMID: 31066084). These are associations, not causation — but they establish the biological plausibility.
What they don't tell you is the dose that works in humans. That's what the clinical trials were supposed to answer.
The First Trial: What the Data Actually Shows
CohBar ran NCT03998514 — a Phase 1a/1b program testing their CB4211 formulation, a stabilized analog of MOTS-c. In the Phase 1a arm, 65 healthy volunteers received escalating subcutaneous doses from 0.2 to 3.0 mg/kg/day for 7 days. The primary endpoint was safety and tolerability. Results: zero serious adverse events. Injection site reactions were the only treatment-emergent event above 10%. The drug was clean.
In Phase 1b, 20 obese patients with NAFLD received 25 mg subcutaneously once daily for 4 weeks. Results presented at AASLD 2021, comparing CB4211 to placebo:
- ALT (liver enzyme) down 25% vs. placebo (p<0.05)
- AST down 17% vs. placebo (p<0.05)
- Fasting glucose down 6% vs. placebo (p<0.05)
- Liver fat content: 33% vs. 36% at baseline; proportion with >30% decrease was 27% vs. 11% placebo
- Body weight: trend toward reduction (p-value not disclosed)
Those aren't pilot-study noise. ALT is a direct marker of hepatic inflammation and stress. Fasting glucose is a direct measure of insulin sensitivity. Both improved simultaneously in 4 weeks at a fixed 25 mg daily dose.
The company published the results. Then they dissolved.
The assets were shopped. Nothing happened. The data sat there — clean, statistically significant, presented publicly — and the company was gone.
The Dose Question: How Did They Get From Mice to Humans?
Animal-to-human dose translation is not guesswork. It is allometric scaling. The standard formula uses the body surface area ratio between species.
- Mouse 0.5 mg/kg/day IP → approximately 3 mg/day human
- Mouse 5 mg/kg/day IP → approximately 28 mg/day human
- Mouse 15 mg/kg three times weekly IP → approximately 85 mg/day human
The 25 mg dose used in the Phase 1b sits squarely in that range. These are not arbitrary numbers. They represent where the biological signal was detectable in animal models before crossing into human testing.
What this means practically: if someone is recommending a MOTS-c protocol, the 5–25 mg/day range is where human safety data exists. Anything above that is extrapolated beyond what the trials have demonstrated. That is not a reason to avoid it. It is a reason to be clear about what the evidence says.
The Second Trial: Running Right Now
Hudson Biotech is running NCT07505745 — a Phase 2a trial in 120 prediabetic patients with BMI 27–40. The protocol specifies "fixed dose once daily for 12 weeks." The exact dose is not disclosed — standard for a masked trial, and frustrating for anyone trying to understand how this compares to the CB4211 data.
Primary endpoint is the OGTT Matsuda Index, a direct measure of whole-body insulin sensitivity. Secondary endpoints include HbA1c, fasting glucose, and body weight. The trial is registered and actively recruiting.
This is the trial that could answer the open questions the CB4211 program left behind. But the results have not been published yet.
So here is the situation as of today: you have a Phase 1b signal in 20 patients showing meaningful improvements in liver enzymes and glucose metabolism, and an ongoing Phase 2a in 120 patients where the data is still being collected.
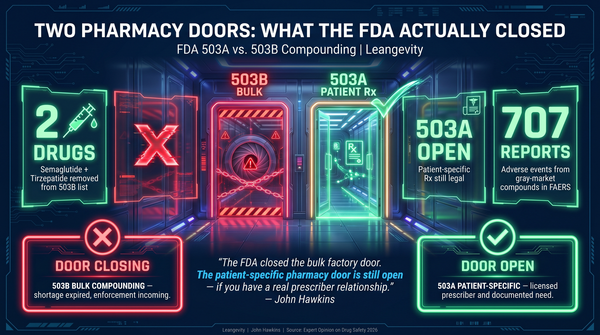
Why July 23 Matters
The FDA's Pharmacy Compounding Advisory Committee meets quarterly to evaluate bulk drug substances for the 503A compounding framework. MOTS-c is on the agenda for the July 23, 2026 meeting.
Currently, MOTS-c sits in FDA 503A Category 2 — compounding is restricted, not prohibited, but the regulatory foundation is contested. A committee recommendation could tighten access significantly or leave the current framework in place.
This matters because compounding access is how most patients access MOTS-c today. Without an FDA-approved product — there is none — compounding is the supply chain.
The committee will be evaluating whether the available evidence supports continued compounding access. The evidence base is: one completed Phase 1b in 20 patients, one ongoing Phase 2a in 120 patients, and a body of animal pharmacology data (PMID: 25738459, PMID: 31293078).
That is not a large evidence base. It is also not nothing.
The Gap Between the Science and the Standard of Care
There is a meaningful difference between biologically plausible and clinically established. MOTS-c has strong mechanistic backing — it activates AMPK, improves insulin sensitivity in animal models, and the human Phase 1b produced a statistically significant signal. That is real.
But a Phase 1b in 20 patients is not a standard of care. It is a signal. The dose range of 5–25 mg/day is supported by the human data. Twice-weekly protocols, higher doses, and oral formulations are not supported by any human trial I have reviewed. If you are seeing those claims elsewhere, ask for the trial number.
Working with a practitioner who knows how to interpret clinical trial data — and who is tracking what happens on July 23 — is not the same as following peptide marketing. That is the practical difference.
What This Means for Patients Currently Using or Considering MOTS-c
The honest answer is: uncertainty.
The science is biologically plausible. MOTS-c acts on metabolic pathways that are well-characterized. The human signal from the CB4211 trial was real. If the Hudson Biotech Phase 2a confirms it, the regulatory conversation changes.
But the human evidence is incomplete. Two trials is not enough to establish a standard of care. The dose question — whether 25 mg daily is optimal, whether twice-weekly is adequate, whether current compounded formulations are bioequivalent to CB4211 — has not been answered.
If you are working with a practitioner on a MOTS-c protocol, the July 23 meeting is worth tracking. A change in compounding status would affect access before year-end.
What To Do With This Information
1. Know the deadline. July 23 is eight weeks away. If you are on MOTS-c or considering it, the regulatory window is closing — or opening — depending on what the committee decides.
2. Evaluate the evidence base honestly. Two human trials. One positive signal. One trial running. The sample sizes are small. The signal is real. The data is not complete.
3. Work with someone who understands the regulatory landscape. The difference between compounding access and a prescription-required product is a committee meeting. That requires knowing what is in the pipeline — not just reading peptide marketing.
4. Do not extrapolate beyond the data. The 5–25 mg/day range is where human safety data exists. Claims outside that range are not supported by the trials. Know the difference.
The math does not care about the hype. Two trials. One regulatory meeting. A decision that affects access for everyone using this peptide right now.
The timeline becomes clear in eight weeks.
References:
- Lee C, et al. Cell Metab. 2015;21(3):443-454. PMID: 25738459
- Kim SJ, et al. Cell Rep. 2019;28(2):581-589.e4. PMID: 31293078
- Gul R, et al. Endocrine. 2019;64(3):512-524. PMID: 31066084
- NCT03998514 — ClinicalTrials.gov (CB4211 Phase 1a/1b, CohBar)
- NCT07505745 — ClinicalTrials.gov (MOTS-MET Phase 2a, Hudson Biotech)
- CohBar AASLD 2021 Poster LB5 — CB4211 Phase 1b Topline Results
Learn more about Leangevity's approach to metabolic optimization at leangevity.fit.
References:
- Lee C, et al. Cell Metab. 2015;21(3):443-454. PMID: 25738459
- Kim SJ, et al. Cell Rep. 2019;28(2):581-589.e4. PMID: 31293078
- Gul R, et al. Endocrine. 2019;64(3):512-524. PMID: 31066084
- NCT03998514 — CB4211 Phase 1a/1b, CohBar
- NCT07505745 — MOTS-MET Phase 2a, Hudson Biotech
- AASLD 2021 Poster LB5 — CB4211 Phase 1b Topline Results
Disclaimer: This content is for educational purposes only. Leangevity provides metabolic health coaching. This is not medical advice, not a prescription, and not a treatment recommendation. Results not typical. Individual results vary. Always consult a qualified healthcare provider before starting, stopping, or modifying any protocol.