Petrelintide: The Weight Loss Drug That Works Without the Nausea
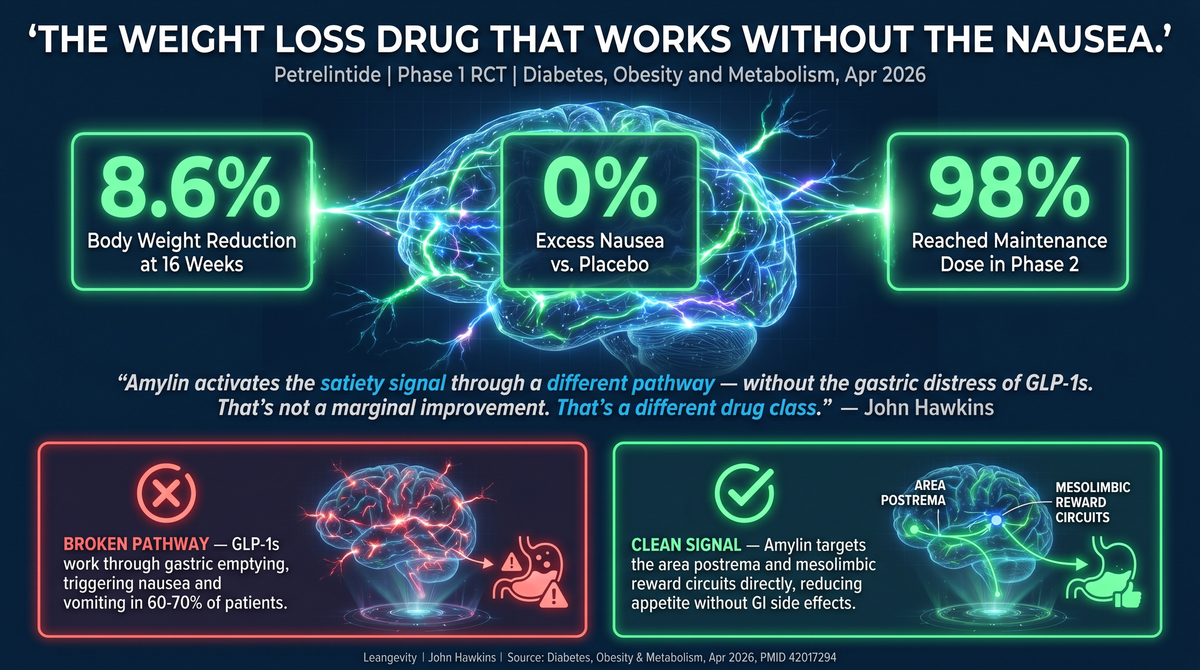
A new amylin analogue (petrelintide) posted Phase 1 results: 8.6% body weight reduction at 16 weeks, nausea rate identical to placebo. Here's what that means for GLP-1 dropouts.
The biggest complaint about GLP-1 weight loss drugs isn't that they don't work. It's that the side effects make people stop taking them.
Up to 60–70% of patients prescribed semaglutide or tirzepatide discontinue within the first year. The reason isn't lack of efficacy — the drugs work. The reason is nausea, vomiting, constipation, and the general feeling of being poisoned every time you eat. Patients call it quits not because they gave up on weight loss, but because the cure felt worse than the condition.
Now there's a new player that might change that equation entirely.
What Is Petrelintide?
Petrelintide is a long-acting amylin analogue developed by Zealand Pharma. Amylin is a peptide hormone co-secreted with insulin from the pancreatic beta cell — but unlike insulin, amylin's primary job is appetite regulation, not glucose management.
It works through two key pathways:
1. Area postrema signaling. The area postrema sits at the base of the brainstem, outside the blood-brain barrier. Amylin reaches it directly, triggering satiety — the feeling of "I'm done eating" — without touching the gut directly.
2. Mesolimbic reward circuit modulation. This is the distinct part. Amylin interacts with the brain's reward pathways in a way that appears to reduce the pull toward hyperpalatable foods without the blunt-force approach of GLP-1 receptor agonism.
The result: reduced caloric intake through a fundamentally different mechanism than GLP-1s. And critically, with a side effect profile that looks almost identical to placebo.
The Data: Phase 1 Results
A pair of randomized, placebo-controlled, double-blind Phase 1 trials published in Diabetes, Obesity & Metabolism (April 22, 2026; PMID 42017294) tested petrelintide in both single ascending dose (SAD) and multiple ascending dose (MAD) protocols.
MAD Part 2 (the obesity trial): 16 once-weekly subcutaneous injections, dose-escalated biweekly to target doses of 2.4mg, 4.8mg, and 9.0mg.
Results:
- Body weight reduction: up to 8.6% after 16 weeks at the highest dose (9.0mg)
- GI adverse events (nausea): 16.7–33.3% across active dose arms vs. 16.7% in the placebo arm
- Only one participant discontinued due to GI adverse events across all dose groups
- No serious or severe treatment-emergent adverse events reported
Let me put that nausea number in plain terms: at the highest dose, petrelintide caused essentially no more nausea than not taking anything at all. Compare that to semaglutide, where nausea rates in clinical trials run 20–44% and real-world discontinuation rates are significantly higher due to GI intolerance.
Phase 2 (ZUPREME-1) topline data: In adults with overweight/obesity, once-weekly petrelintide achieved up to 10.7% body weight reduction at 42 weeks, with 98% of participants reaching the maintenance dose — meaning almost everyone tolerated it well enough to stay on therapy.
Why the GI Tolerability Difference?
The short answer: different mechanisms, different side effect profiles.
GLP-1 agonists cause GI distress through multiple mechanisms — delayed gastric emptying (the food sits in your stomach too long), increased gut motility signaling, and direct stimulation of the vomiting reflex. The same mechanism that makes you feel full also makes you feel sick.
Amylin's satiety signal originates in the brain, not the gut. It doesn't slow gastric emptying in the same way. Patients feel less hungry without the visceral discomfort of a GLP-1.
This doesn't mean petrelintide is automatically better for everyone. Amylin-based therapies carry their own considerations — notably, the theoretical concern about amylin's effects on gastric acid secretion (amylin normally suppresses gastric acid as a satiety signal). But the Phase 1 safety profile is clean, and the GI tolerability advantage is real.
The Practical Implications
1. The GLP-1 dropout problem is massive. The single largest gap in obesity pharmacotherapy isn't new drug development — it's patient retention. Millions of people started a GLP-1, felt terrible, and quit. Many of them gained the weight back. Petrelintide offers a credible pharmacological off-ramp for this population.
2. Combination therapy is the next frontier. Amylin and GLP-1 work through complementary pathways. Cagrilintide (amylin analogue) + semaglutide combinations have already shown additive weight loss in earlier trials. Petrelintide's clean tolerability profile makes it an ideal candidate for future dual-agonist or combination approaches.
3. Once-weekly dosing matters. A drug you tolerate perfectly but can't stay on is useless. A drug you tolerate perfectly and can stay on is a protocol. Petrelintide's ~10-day half-life supports true once-weekly dosing with minimal dose titration burden.
The Bottom Line
Here's what's actually happening metabolically: the GLP-1 class changed the game for obesity pharmacotherapy, but the GI tolerability problem created a secondary problem — a large, frustrated population who tried the standard of care and couldn't stay on it.
Petrelintide, if Phase 3 data holds, may solve that problem. Competitive weight loss — 8.6% at 16 weeks, 10.7% at 42 weeks — with a GI tolerability profile essentially indistinguishable from placebo. That's not a marginal improvement. That's a meaningful differentiation.
The competitive landscape is shifting fast. Phase 2 results from ZUPREME-1 read out in March 2026. The window to position yourself as the voice that understands this space — before mainstream health media catches up — is right now.
If you're comparing obesity pharmacotherapy options, or if you've tried and stopped a GLP-1 due to side effects, understanding the amylin pathway is worth your time. This is one of the more significant developments in metabolic pharmacology in recent years.
Sources
- Blundell J, et al. "Petrelintide, a long-acting amylin analogue, in adults with overweight or obesity: a phase 1 randomized controlled trial." Diabetes, Obesity & Metabolism. April 22, 2026. PMID: 42017294
- Supplementary: PMID 41793055 — Comprehensive Physiology review on brain amylin signaling (April 2026)
- Zealand Pharma press release: ZUPREME-1 Phase 2 topline results (March 2026)
Leangevity provides metabolic health coaching, not medical treatment. This content discusses emerging research and is not a treatment recommendation. Consult your healthcare provider before starting, stopping, or changing any medication protocol.