Your Psoriasis Isn't a Skin Problem. The Evidence Points Somewhere Else.
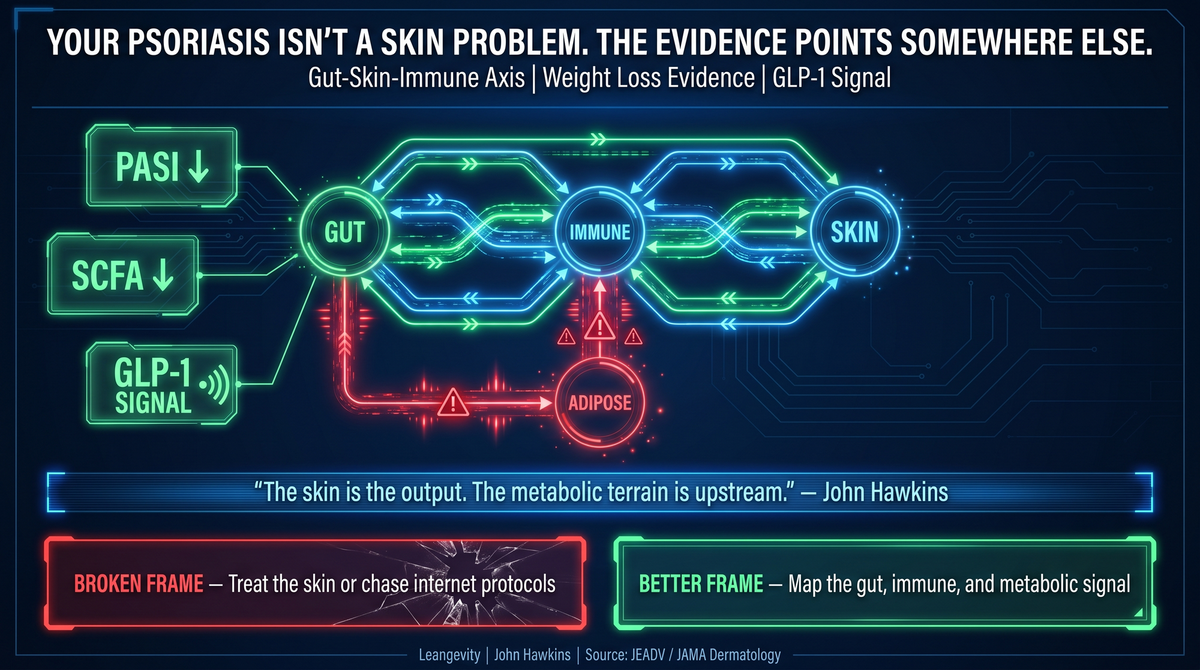
Psoriasis looks like a skin problem, but the strongest human evidence points upstream: gut-immune signaling, metabolic state, and weight loss.
Published by Leangevity | Evidence-based metabolic coaching
Millions of people with psoriasis have been told two things. Get on a biologic and manage the symptoms. Or heal your gut with the right elimination diet, the right probiotic, and the right internet protocol.
Both camps have a piece of the picture. Neither one has the whole thing.
Here is what the evidence actually shows — and why the most actionable lever for psoriasis severity is one that almost nobody brings to patients in plain language.
The Skin Is Not Where This Starts
Psoriasis looks like a skin problem. The plaques, the scaling, the inflammation — that is where patients feel it and where most treatment aims.
The skin is not the origin. It is the endpoint.
The upstream chain looks like this: gut bacteria fall out of balance, the intestinal wall weakens, and bacterial toxins called lipopolysaccharides (LPS) leak into the bloodstream. Those toxins activate immune cells — specifically the IL-23/Th17 immune axis, the central driver of psoriatic inflammation confirmed across clinical trial reviews (PMID 38616886).
When IL-23 is elevated, it pushes Th17 cells to produce IL-17A. IL-17A drives skin cells to proliferate and generate the inflammatory plaques that define psoriasis.
This is not a fringe theory. It is the same pathway that the most advanced biologics target. The difference is that dermatology's tools hit the axis near the end. They suppress IL-17 or IL-23 directly. That works — but it is downstream of where the signal originated.
The gut is upstream.
What the Gut Actually Has to Do With It
Two comprehensive 2026 reviews map the gut-skin connection directly.
Andrzejczak et al. (PMID 41972685, Cells 2026) documents the bidirectional gut-skin network: gut dysbiosis feeds the Th17/IL-23 cycle through reduced short-chain fatty acid (SCFA) production, altered microbial metabolites, and systemic immune activation.
Yahyapour et al. (PMID 41568321, J Transl Autoimmunity 2026) confirms the specific bacterial pattern. Psoriasis patients consistently show reduced populations of Faecalibacterium and Akkermansia — two protective species that maintain gut barrier integrity and regulate immune tone — and increased pro-inflammatory bacteria.
Fewer protective bacteria means less barrier protection. Less barrier protection means more LPS entering the bloodstream. More LPS means more IL-23 activation. More IL-23 means more skin inflammation.
The mechanism connects.
But knowing the gut is involved is not enough anymore. That framing is already everywhere — functional medicine sites, Healthline, naturopathic channels. Every wellness account has a leaky gut explainer. The question the research actually answers is: what intervention has the strongest human evidence for reducing psoriasis severity?
That answer is not where most people are looking.
Where the Natural-Health World Goes Wrong
The functional medicine and wellness space got the upstream intuition right. Psoriasis is not just a skin problem. The gut and immune system are involved upstream.
The problem is what comes next.
Search for psoriasis on Reddit, TikTok, or any natural-health site and you will find carnivore diets producing dramatic remissions (no randomized controlled trials exist), AIP protocols reversing the condition (no RCTs), beef tallow as a topical treatment (no clinical evidence), DMSO, low-dose naltrexone, peptide injections. Every week brings a new protocol.
The published human evidence includes zero randomized controlled trials showing remission from these approaches in patients trying to make real treatment decisions. The anecdotes may be real experiences. They are not clinical evidence. And presenting them as such is a mistake — one the wellness side makes consistently.
When patients follow unverified protocols instead of addressing proven metabolic drivers, they are not doing nothing. They are often delaying the interventions with actual evidence behind them.
There is also a cost to hope spent on the wrong thing. Psoriasis has a real genetic component — true remission is not guaranteed by any protocol. But severity, quality of life, and inflammatory burden are meaningfully modifiable. That is worth knowing before spending years cycling through elimination protocols that have never been tested in a controlled trial.
The Strongest Evidence Points to Weight Loss
This is the finding that is almost entirely absent from patient-facing psoriasis content.
A 2025 systematic review and meta-analysis published in JEADV (PMID 41416383) evaluated weight-loss interventions in psoriasis patients with excess weight. Weight loss consistently improved PASI scores — the standard measure of psoriasis area and severity — and improved quality of life.
This is A-grade evidence. It is stronger than any supplement data and stronger than any diet-protocol observational study. It lives in academic journals while patients are on Reddit debating which elimination diet worked for someone's cousin.
The metabolic-severity link is not subtle. Excess adiposity is associated with more severe disease and worse inflammatory burden (PMID 41416383, PMID 41468253). Fat tissue is not passive storage. It is an endocrine organ. It secretes inflammatory signals — adipokines, TNF-alpha, IL-6 — that feed directly into the same immune cascade that drives skin lesions (PMID 41839448).
The extra adipose tissue is actively amplifying the psoriasis. Via the same inflammatory pathways that biologics target downstream.
This is not a theory. It is a pattern in A-grade evidence that rarely gets translated into language patients can act on.
The GLP-1 Signal Is Worth Paying Attention To
In 2026, the National Psoriasis Foundation published a primer in JAMA Dermatology (PMID 42054048) reviewing GLP-1 receptor agonist data in psoriasis patients.
The individual studies are small — N=7 to N=48, short-term, mostly uncontrolled. This is not practice-changing evidence and it is not a treatment recommendation.
What it is: another signal that psoriasis and metabolic state are deeply connected. GLP-1 receptor agonists were designed to correct metabolic dysfunction. They reduce visceral fat, improve insulin sensitivity, and lower systemic inflammation. When those same drugs also reduce psoriasis severity by 40-80% in early cohort data, the pattern points at the same upstream metabolic driver the weight-loss trials identified.
When a major dermatology organization publishes a formal primer because the metabolic-psoriasis signal is strong enough to formalize, that tells you something about the direction the evidence is moving.
The skin was always downstream. The metabolic terrain was always upstream.
What the Evidence-Based Middle Actually Looks Like
There is a space between "take your biologic and don't ask questions" and "drink this supplement stack and heal your gut."
That space is metabolic coaching grounded in what the evidence supports.
The interventions with the strongest human evidence for psoriasis severity in people carrying excess weight are not exotic. Weight loss through metabolic correction reduces the adipose inflammatory burden and improves insulin sensitivity. Mediterranean diet adherence is associated with lower psoriasis severity in case-control data (PMID 41468253). The pattern fits the broader metabolic picture.
Omega-3 fatty acids have relevant evidence. A 2025 Mendelian randomization study (PMID 40843457) provides causal genetic evidence that DHA reduces psoriasis risk. A 2026 systematic review (PMID 41534196) confirms clinical observations of omega-3 effects on psoriatic lesions.
A 2025 network meta-analysis of 21 RCTs including 1,463 patients (PMID 41459063) supports adjunctive roles for dietary supplements in psoriasis management.
These are not miracle protocols. They are supportive interventions with human evidence behind them. One category has clinical trials. The other has social media posts. The distinction matters when you are the one living with psoriasis.
None of these replace a physician. Psoriasis requires medical evaluation and ongoing care. Metabolic coaching works alongside that — not instead of it.
The Question Worth Asking
If your psoriasis has been managed at the symptom level and the upstream terrain — metabolic health, gut function, inflammatory burden, body composition — has never been part of the conversation, that is worth examining.
The evidence on what drives severity upstream is stronger than most patients realize. And it points at levers that conventional dermatology often does not have time to address.
If you are dealing with psoriasis alongside excess weight or metabolic dysfunction and want to understand the connections the research supports, a physician-supervised metabolic coaching program is a reasonable place to start that conversation.
Start here: leangevity.fit
Medical disclaimer: This article is for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Psoriasis is a medical condition requiring physician evaluation and management. Do not change, stop, or start any treatment based on this content. Consult your physician before making any changes to your health plan.
Sources:
- Potestio et al. (2024). IL-23/17 axis in psoriasis management. PMID 38616886
- Andrzejczak et al. (2026). Gut dysbiosis and gut-skin axis in psoriasis. Cells. PMID 41972685
- Yahyapour et al. (2026). Gut microbiome in psoriasis. J Transl Autoimmunity. PMID 41568321
- Impact of weight-loss interventions on psoriasis severity: SR+MA. JEADV 2025. PMID 41416383
- Mediterranean diet, obesity, and disease severity in psoriasis. Nutr Health 2025. PMID 41468253
- Immunometabolic dysregulation in psoriasis. Immunol Invest 2026. PMID 41839448
- National Psoriasis Foundation primer on GLP-1 RAs in psoriasis. JAMA Dermatology 2026. PMID 42054048
- Causal effect of plasma fatty acid profiles on psoriasis risk: MR study. PMID 40843457
- Therapeutic approach with fatty acids in psoriasis: SR. Aten Primaria 2026. PMID 41534196
- Dietary supplements in psoriasis: network meta-analysis, 21 RCTs, N=1,463. Frontiers Nutrition 2025. PMID 41459063